

Summary
Hypertensive individuals, who cannot achieve target blood pressure (BP) levels despite being treated with triple-drug regimens, including a diuretic, are diagnosed as having resistant hypertension (rHT) [Calhoun DA et al. Circulation 2008], which is an increasingly common clinical problem [Egan BM et al. Circulation 2011]. Renal sympathetic hyperactivity is influential in the maintenance and progression of hypertension, while the interruption of sympathetic nerves in the kidney has a strong impact on BP and survival. This article discusses the impact of renal denervation as a treatment for hypertension.
- Cardiometabolic Disorder
- Interventional Radiology Hypertensive Disease
- Interventional Techniques & Devices
- Diabetes & Kidney Disease
- Hypertension & Kidney Disease
- Renal Disease
- Renal Disease
Hypertensive individuals, who cannot achieve target blood pressure (BP) levels despite being treated with triple-drug regimens, including a diuretic, are diagnosed as having resistant hypertension (rHT) [Calhoun DA et al. Circulation 2008], which is an increasingly common clinical problem [Egan BM et al. Circulation 2011]. rHT is believed to be caused by over- and chronic activation of the sympathetic nervous system. Renal sympathetic hyperactivity is influential in the maintenance and progression of hypertension, while the interruption of sympathetic nerves in the kidney has a strong impact on BP and survival. Michael Böhm, MD, Universitätsklinikum des Saarlandes, Saarbrücken, Germany, discussed the impact of renal denervation as a treatment for hypertension.
A better understanding of renal nerve anatomy has enabled the use of a catheter-based radio frequency approach for the ablation of nerves using a standard interventional technique. The Renal Denervation in Patients with Refractory Hypertension [Symplicity HTN-1; NCT00664638] study established the safety and proof-of-principle for catheter-based renal sympathetic denervation in patients with rHT In the study, 95% of patients experienced significant reductions in BP, which were sustained for 24 months without significant adverse events. There was no evidence of the development of tolerance or re-enervation. In the Symplicity HTN-2 [NCT00888433] study, the primary endpoint was change in seated office-based systolic BP (SBP). At 6 months, 41 (84%) of 49 patients who underwent renal denervation had a reduction in SBP of 10 mm Hg or more compared with 18 (35%) of 51 controls (p<0.0001) [Symplicity HTN-2 Investigators. Lancet 2010].
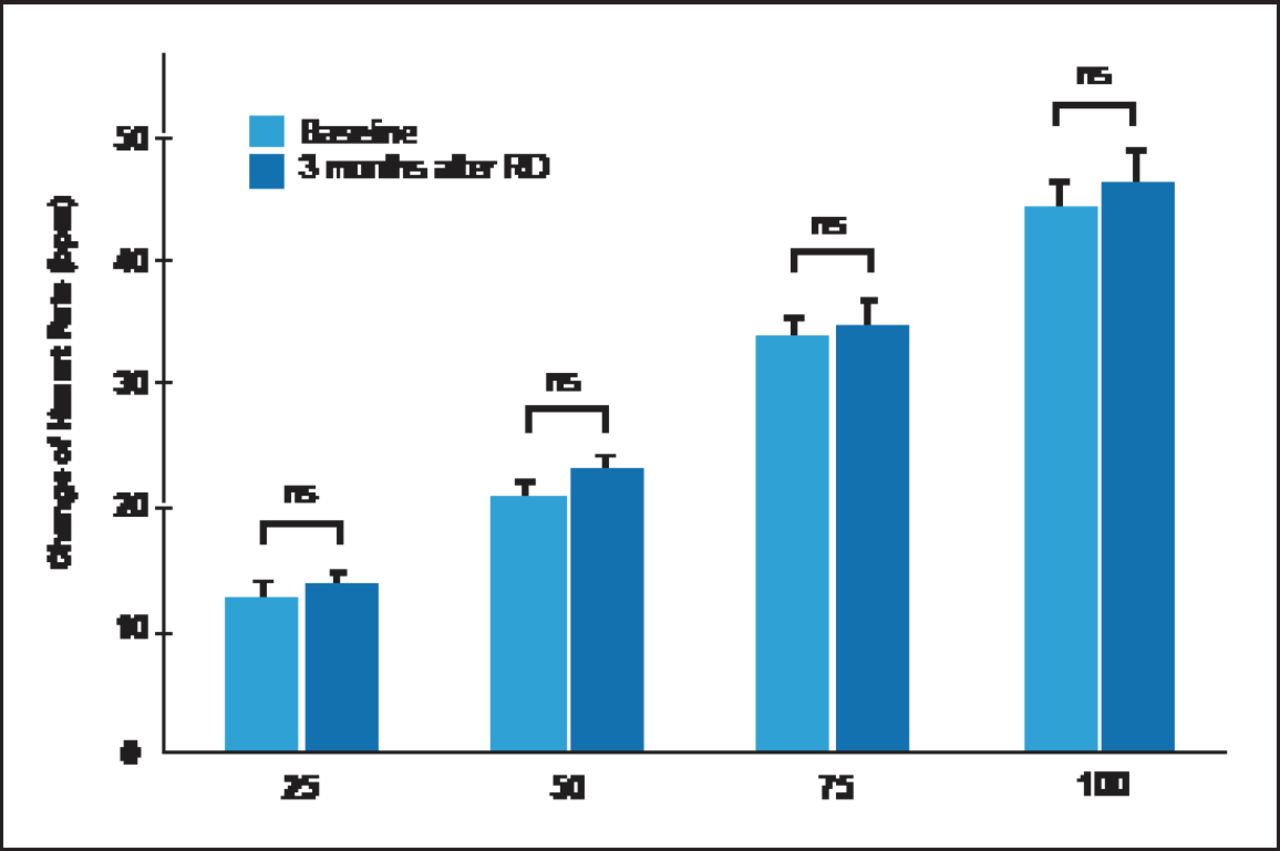
In an extension of the Symplicity HTN-2 study, investigators assessed the effects of renal denervation on cardiorespiratory response to exercise. The results showed that BP during exercise was reduced, heart rate at rest decreased, and heart rate recovery improved (Figure 1) [Ukena C et al. J Am Coll Cardiol 2011]. In addition to its known effect on BP, renal denervation has also been shown to significantly reduce left ventricular mass and improve diastolic function, which might have important prognostic implications in patients with resistant hypertension at high cardiovascular risk [Brandt MC et al. J Am Coll Cardiol 2012].

Heart Rate Change During Exercise.
RD=renal denervation. Reprinted from Ukena C et al. Cardiorespiratory response to exercise after renal sympathetic denervation in patients with resistant hypertension. J Am Coll Cardiol. 2011 Sep 6;58(11):1176–82, with permission from Elsevier.
Luis M. Ruilope, MD, Hospital 12 de Octubre, Madrid, Spain, discussed the prevalence, treatment, and risk factors for rHT.
Data from the National Health and Nutrition Examination Survey [NHANES] found that rHT increased from 15.9% (1988 to 2004) to 28.0% (2005 to 2008) of treated patients (p<0.001) [Egan BM et al. Circulation 2011]. However, another study found the percentage to be as low as 12.2%, of which only 7.6% was true rHT (the remaining 4.6% was “white-coat” hypertension) [de la Sierra A et al. Hypertension 2011]. Part of the problem with identifying rHT is how BP is measured. The best method for a correct diagnosis is likely 24-hour ambulatory BP monitoring (ABPM), particularly in diabetic patients [Gorostidi M et al. Hypertens Res 2011]. Twenty-four-hour ABPM can identify variations in BP levels throughout the day and eliminate the white-coat effect. High ABPM values are associated with worse prognosis in rHT patients, as well as higher incidence of cardiovascular events.
rHT is almost always multifactorial in etiology. In addition to obesity and diabetes, excessive salt consumption is an important contributor, hence strategies to reduce dietary salt intake should be part of the overall treatment plan [Pimenta E et al. Hypertension 2009]. Secondary causes include obstructive sleep apnea (OSA), renal parenchymal disease, primary aldosteronism, and renal artery stenosis [Calhoun DA et al. Hypertension 2008]. Once it has been determined that the patient has truly resistant hypertension (pseudoresistance has been ruled out, lifestyle- and medication-related issues have been eliminated, and secondary causes of rHT have been excluded) a pharmacologic approach should be developed. At present the most effective treatment paradigm appears to be triple-combination drug therapy [Calhoun DA et al. Hypertension 2009]. In patients uncontrolled by triple therapy, spironolactone has been shown to be effective in lowering BP [Chapman N et al. Hypertension 2007; Alvarez-Alvarez B et al. J Hypertension 2010].
rHT is highly prevalent and frequently accompanied by other cardiovascular risk factors. Prof. Ruilope concluded that, following failed pharmacological therapy, renal denervation should play a role in its treatment.
Felix Mahfoud, MD, Universitätsklinikum des Saarlandes, Saarbrücken, Germany, discussed the topics of glucose metabolism, insulin resistance, heart failure, and OSA in relation to renal denervation.
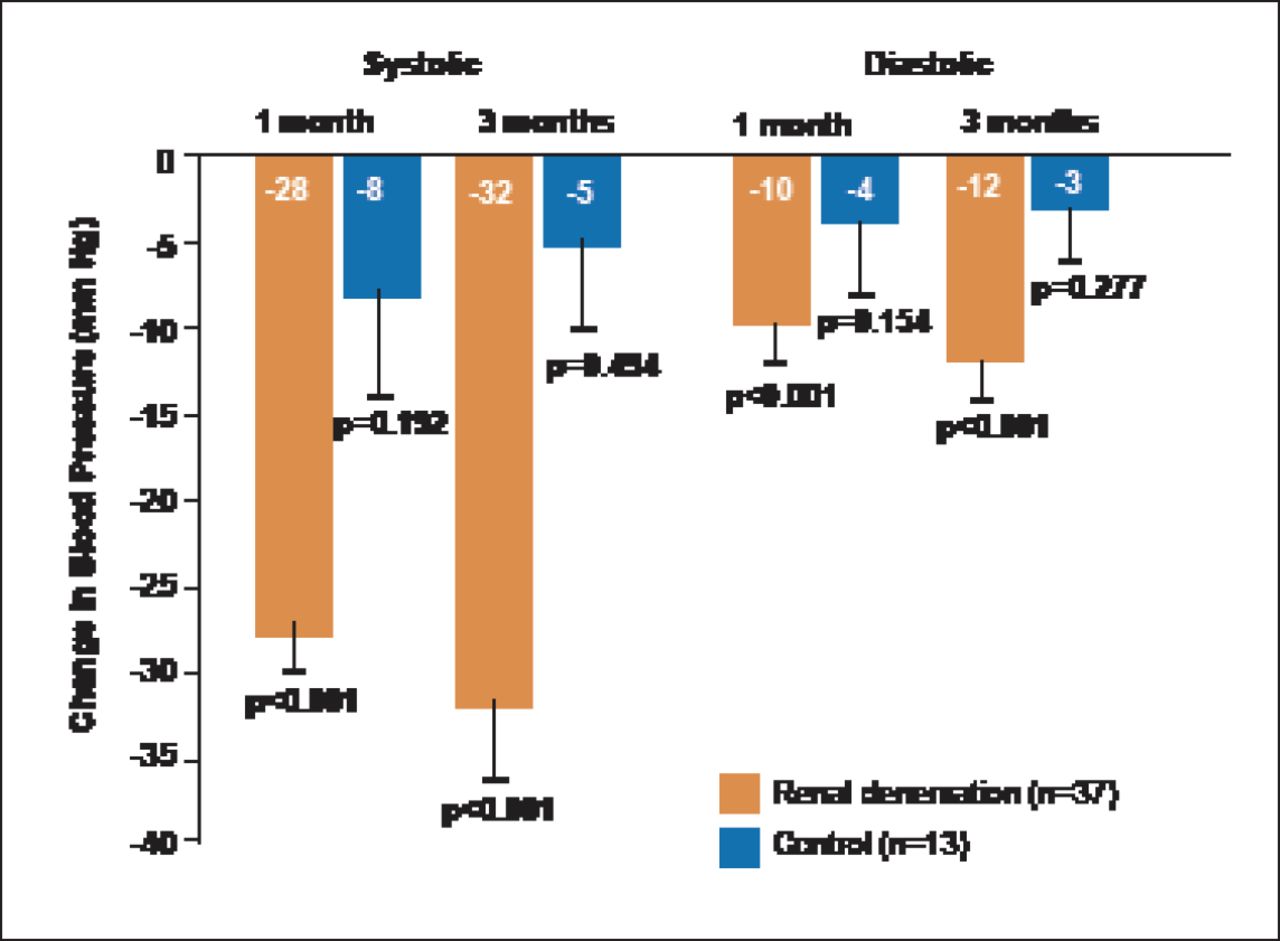
In a pilot study in patients with rHT, renal denervation reduced fasting, mean 2-hour glucose and C-peptide levels, and insulin sensitivity, in addition to significantly reducing BP (Figure 2), suggesting that the procedure may provide protection for patients with rHT and metabolic disorders who are at high cardiovascular risk [Mahfoud F et al. Circulation 2011]. Studies have also shown that bilateral renal nerve ablation is associated with substantial improvement in insulin sensitivity, while reducing glomerular hyperfiltration and urinary albumin excretion [Schlaich MP et al. J Hypertens 2011] and improving glucose tolerance [Witkowski A et al. Hypertension 2011].

BP Reduction After Renal Denervation.
Reprinted from Mahfoud F et al. Effect of Renal Sympathetic Denervation on Glucose Metabolism in Patients With Resistant Hypertension: A Pilot Study. Circulation. 2011;123:1940–1946, with permission from Lipincott Williams and Wilkins.
Sympathetic activity correlates to NYHA class and heart failure, while chronic heart failure (CHF) is characterized by increased sympathetic activity, which is proportional to severity of CHF. Cardiac norepinephrine spillover increased 3-fold in mild to moderate CHF patients and 4-fold in severe CHF patients. This indicates increased amounts of transmitter available at neuroeffector junctions that precede the augmented sympathetic outflow to the kidneys and skeletal muscle found in advanced CHF. Because previous research suggests that the kidneys are a major contributor to heart failure, a study of the effects of sympathetic renal denervation in patients with CHF is in progress.
OSA is associated with sympathovagal imbalance, atrial fibrillation, and postapneic BP increases. Renal denervation displays antiarrhythmic effects by reducing negative tracheal pressure–induced atrial effective refractory period shortening, and it inhibits postapneic BP increases associated with OSA-associated AF [Linz D et al. Hypertension 2012]. The safety of renal denervation was demonstrated in a study that showed the procedure reduced BP, renal resistive index, and the incidence of albuminuria without adversely affecting glomerular filtration rate or renal artery structure [Mahfoud F et al. Hypertension 2012].
Prof. Mahfoud suggested that patients with the following characteristics are suitable for renal denervation:
-
SBP ≥160 mm Hg (≥150 mm Hg for type 2 diabetes patients)
-
≥3 antihypertensive drugs in adequate dosage and combination (including diuretic)
-
Completion of life-style modifications (eg, diet)
-
Exclusion of secondary hypertension
-
Exclusion of pseudoresistance (eg, via 24-hour ABPM)
-
Preserved renal function (estimated glomerular filtration rate ≥45 mL/min/1.73 m2)
-
Eligible renal arteries: no stenosis, no percutaneous transluminal angioplasty/stenting
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.