

Summary
Stephen MacMahon, MD, DSc, George Institute for Global Health at the University of Sydney, Sydney, Australia, presented the Lewis A. Conner Memorial Lecture. The theme of Prof. MacMahon's presentation was frugal innovation, an approach he believes will be essential for the future of cardiovascular medicine in the 21st century. “Despite the many innovations in the treatment and prevention of cardiovascular disease, the benefits have been felt by few of the many individuals that are actually in need,” said Prof. MacMahon.
- Prevention & Screening
Stephen MacMahon, MD, DSc, George Institute for Global Health at the University of Sydney, Sydney Australia, presented the Lewis A. Conner Memorial Lecture. The theme of Prof. MacMahon's presentation was frugal innovation, an approach he believes will be essential for the future of cardiovascular (CV) medicine in the 21st century. “Despite the many innovations in the treatment and prevention of cardiovascular disease [CVD], the benefits have been felt by few of the many individuals that are actually in need,” said Prof. MacMahon.
A major challenge today is how to provide basic care for the 7 billion people on the planet, 3 billion of whom are likely to develop serious CVD sometime in their life. Currently, 5 billion individuals have no reliable access to essential CV health care. In a study conducted in India, the prevalence of coronary heart disease (CHD) and cerebrovascular disease was estimated to be 4.8% and 2.0%, respectively. Among individuals with either diagnosis, 14% reported taking aspirin, 41% took a blood pressure-lowering medication, and only 5% reported using a cholesterol-lowering medication [Joshi R et al. Circulation 2009].
Similar findings were reported in the Prospective Urban Rural Epidemiological [PURE] study, in which the use of secondary prevention medications was low worldwide but especially in low-income countries and rural areas [Yusuf S et al. Lancet 2011]. Many people in the world with serious CVD receive no treatment whatsoever because most of the world's high-risk individuals live in resource-poor regions. Of the individuals who are at risk of CVD, 80 million live in high-income regions and 250 million live in the rest of world. Those in the high-income areas have access to a CV drug budget of $100 billion compared with <$20 million in the poorer regions. The same disparity holds true for quality of care and the distribution of physicians. Cost is another major issue. In a study in China, workers without health insurance were 7 times more likely to experience catastrophic payments (defined as ≥30% of total household annual income) than workers with insurance [Heeley E et al. Stroke 2009].
There are vast numbers of unmet CV healthcare needs that are related to inadequate workforce and resources. There is a great variation in the global quality of care and high cost relative to the ability to pay. Consequently, many tens of millions of individuals die prematurely and unnecessarily every decade from preventable CV causes. Radical action is needed to avert this consequence. Prof. MacMahon proposed the need to embrace the notion of frugal innovation, which includes solutions that are affordable to the >3 billion individuals living on less than $2.50/day. These innovations need to be economically disruptive and lead to fundamental market changes, ie, a model that is low margin, high volume.
Prof. MacMahon discussed three frugal innovation approaches that might help alleviate the unmet needs for CVD prevention and treatment.
Primary care workforce models developed in high-income countries are impractical and unaffordable elsewhere. Physician-centered care is not the solution as there are too few physicians, and they are too expensive, difficult to retain, and display a wide variation in the quality of care. For example, there are 500,000 doctors in India today; if India were to adopt a US-style approach to health care, 3 million physicians would be required.
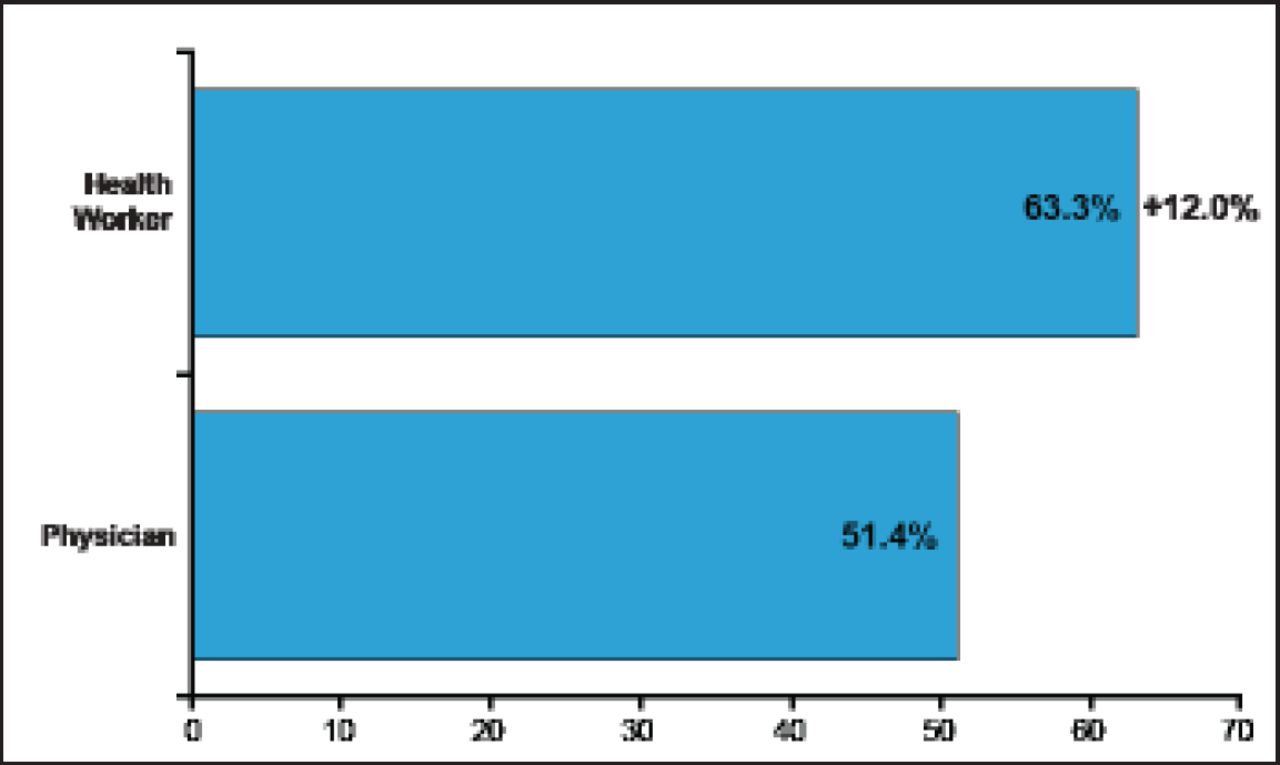
To meet the demands of individuals in low-income regions, the medical workforce needs to be larger and more affordable, and deliver care with consistent quality. An alternative is to equip and train an allied work force to provide basic, essential cardiac care. In a government-funded program in India, high school graduates were trained to be multipurpose health workers. They were trained using an algorithm-based screening and treatment approach for secondary prevention and high-risk primary prevention of CVD, the leading cause of death in India. These workers were able to detect and identify high-risk individuals at a higher rate than physicians. There was also good agreement between the health workers and physicians regarding treatment of patients with CHD, ie, the prescribing of angiotensin-converting enzyme inhibitors, β-blockers, statins, and aspirin (Figure 1) [Joshi R et al. J Am Coll Cardiol 2012]. There is a similar program ongoing in China for patients at high risk of stroke.

Identification of High-Risk Individuals by Multipurpose Healthworker.
Adapted from S MacMahon, MD. AHA 2012.
Another approach is the development of low-cost technologies, in part to facilitate the expansion of the medical work force, but also to improve the quality of care. The Systematic Medical Assessment Referral and Treatment (SMART) program is an example of an electronic decision support system used for patient assessment, diagnosis, treatment, follow-up, referral, and quality control regarding primary and secondary prevention of stroke, heart disease, and kidney disease. Low-cost remote electronic sensors for mobile phones are being developed that can collect a range of information regarding CV markers, eg, blood pressure, heart rate, electrocardiogram, and heart sounds. Another technological development underway is consumer devices for monitoring CV risk, early warning signs, and symptoms. These devices also contain programs that remind patients to take medication, keep track of weight loss, choose healthy foods, and schedule appointments.
Pharmaceutical innovation is particularly important for emerging markets. Low-cost drugs in fixed-dose once-a-day combinations can help meet the demands for drugs in low-income regions. This requires a shift to low margins with high volume. Efforts are underway to develop drugs that are low-cost, fixed-dose, once-a-day combinations for CVD. The Programme to Improve Life and Longevity [PILL] pilot study conducted by Prof. MacMahon was a 12-week placebo-controlled trial using a fixed-dose combination pill for stroke prevention [PILL Collaborative Group. PLoS ONE 2011]. The pill was a combination of aspirin (75 mg), simvastatin (20 mg), lisinopril (10 mg), and hydrochlorothiazide (12.5 mg) taken daily. The estimated effects for patients continuing long-term treatment of the combined pill produced included a ∼60% reduction for risk of CHD and ischemic stroke (Table 1) at a cost significantly less than the sum of the individual ingredients.
Estimated Reductions in Cardiovascular Risk for Those Remaining on Treatment.
Ongoing efforts like these have the potential to reduce the disease burden while preventing a sharp rise in worldwide costs.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.