

Summary
This article reviews the current treatment approaches and emerging therapies for atrial fibrillation.
- Interventional Techniques & Devices
- Arrhythmias
There are an estimated 2.2 million people in the United States with atrial fibrillation (AF). Approximately 70% of these individuals are aged between 65 and 85 years. The prevalence of AF is 2.3% in people aged >40 years and 5.9% in those aged >65 years [Feinberg MW et al. Arch Intern Med 1995]. AF in patients with heart failure (HF) increases from <10% in those who are classified as New York Heart Association (NYHA) functional class I to approximately 50% in NYHA functional class IV patients [Maisel WH et al. Am J Cardiol 2003].
Catheter ablation is a successful procedure for the treatment of AF in appropriately selected patients, more for paroxysmal compared with persistent/permanent AF. Single and multiple procedure success rates are between 60% to 75% and 70% to 85%, respectively. The current approach to performing ablation is to create continuous lesions that encircle the ipsilateral pulmonary vein, placed with irrigated radiofrequency energy to prevent microreentry and, hence, atrial arrhythmias. Raul Mitrani, MD, University of Miami, Miami, Florida, USA, reviewed the current treatment approaches and emerging therapies for AF.
In their 2011 focused update for maintenance of sinus rhythm, the American College of Cardiology/American Heart Association/Heart Rhythm Society (ACC/AHA/HRS) modified or added new recommendations concerning the use of catheter ablation for the maintenance of sinus rhythm [Wann LS et al. Circulation 2011].
Modified recommendations
-
Catheter ablation, performed in experienced centers (>50 AF catheter ablations/year) is useful in maintaining sinus rhythm in selected patients with significantly symptomatic, paroxysmal AF who have failed treatment with an antiarrhythmic drug and have normal or mildly dilated left atria, normal or mildly reduced left ventricular (LV) function, and no severe pulmonary disease (Class I; Level of Evidence [LOE]: A)
-
In patients with AF without structural or coronary heart disease, initiation of propafenone or flecainide can be beneficial on an outpatient basis in patients with paroxysmal AF who are in sinus rhythm at the time of drug initiation. (Class IIa; LOE: B)
New recommendations
-
Catheter ablation is reasonable to treat symptomatic persistent AF. (Class IIa; LOE: A)
-
Catheter ablation may be reasonable to treat symptomatic paroxysmal AF in patients with significant left atrial dilatation or with significant LV dysfunction. (Class IIb; LOE: A)
Dr. Mitrani reviewed data from several ablation studies, some of which were cited by the ACC/AHA/HRS as contributing to the revised recommendations. Wilber et al. reported results from a prospective, multicenter study that compared catheter ablation with antiarrhythmic drug therapy (ADT) in 167 patients with symptomatic paroxysmal AF who did not respond to at least one antiarrhythmic drug and who experienced at least 3 AF episodes within 6 months before randomization. At 9 months, 66% of patients in the catheter ablation group remained free from protocol-defined treatment failure (documented symptomatic paroxysmal AF during the effectiveness evaluation period; repeat ablation after Day 80 of the initial ablation, absence of entrance block confirmed in all pulmonary veins at the end of the ablation procedure, or changes in specified drug regimen postblanking were also considered treatment failures as were adverse events requiring discontinuation of the assigned drug in the ADT group) compared with 16% of patients who were treated with ADT (HR, 0.30; 95% CI, 0.19 to 0.47; p<0.001). Major 30-day treatment-related adverse events occurred in 5 of 57 patients (8.8%) who were treated with ADT and 5 of 103 patients (4.9%) who were treated with catheter ablation. Mean quality of life scores improved significantly (p<0.001) in patients who were treated by catheter ablation compared with ADT at 3 months; improvement was maintained during the course of the study [Wilber DJ et al. JAMA 2010]. Support for ablation also comes from a meta-analysis of 35 studies, in which radiofrequency ablation was more effective at preventing AF compared with ADT in either paroxysmal or persistent AF [Parkash R et al. J Cardiovasc Electrophysiol 2011]. In another study, catheter ablation of AF was effective in approximately 80% of patients after 1.3 procedures per patient, with approximately 70% of patients not requiring further ADT during intermediate follow-up [Cappato R et al. Circ Arrhythm Eledctrophysiol 2010].
Finally, Ouyang and colleagues showed that long-term circumferential pulmonary isolation results in stable sinus rhythm in the majority of appropriately selected patients with paroxysmal AF and normal LV function, and a low incidence of recurrent AF was noted after 5 years of follow-up [Ouyang F et al. Circulation 2010]. The long-term recurrence rate for AF after an initially successful ablation is secondary to electrical reconnection from the pulmonary veins; hence, a repeat ablation may restore sinus rhythm.
The existing focal catheter technology has been adapted to isolate pulmonary veins and ablate atrial tissue. For focal catheters that are not specifically designed for pulmonary vein isolation, there are still challenges: good lesions require transmurality; cardiac contractions make maintaining position difficult; patient anatomy is variable; atrial tissue depth is variable; catheter force varies with position in the heart; and successful procedures require contiguous lesions.
Newer approaches, such as cryoablation, use a balloon and freezing. The Arctic Font® Cardiac CyroAblation Catheter System creates a circumferential, transmural lesion by removing heat from the tissue, leading with a wave of hypothermia, with the coldest temperatures contained within the ablation zone around the balloon, which ablates at the point of tissue contact.
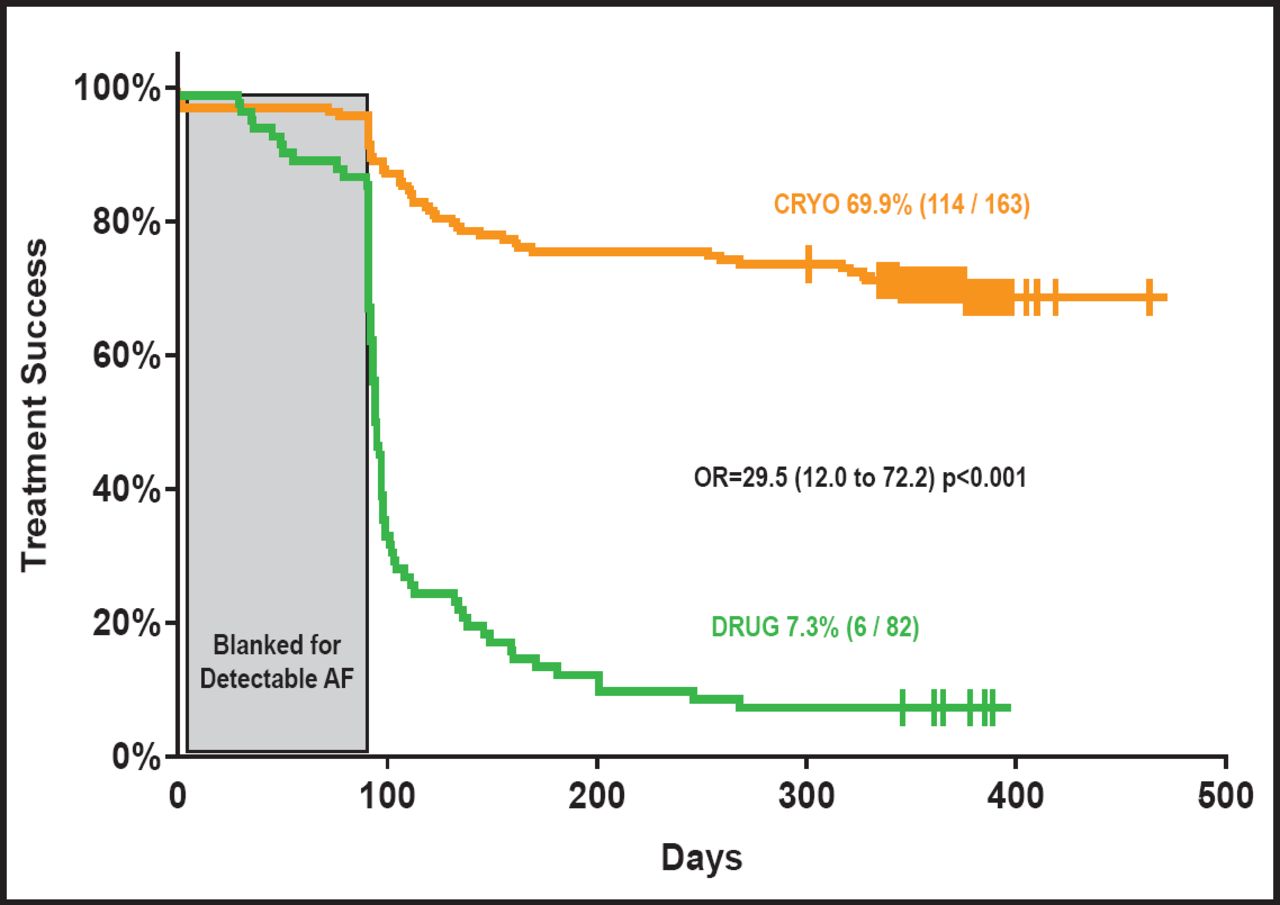
The STOP AF (clarify randomized, nonrandomized) (Sustained Treatment of Paroxysmal Atrial Fibrillation) trial compared ablation with the Arctic Front system and ADT in 245 patients with paroxysmal AF. To be eligible, patients were required to have experienced at least 2 episodes of AF within 2 months, as documented by ECG, or to have failed at least one antiarrhythmic drug. The study population was relatively young (mean age 56 years), with a mean CHADS2 score of 0.6. Patients were followed for 12 months, with 69.9% of patients who were treated with cryoablation achieving the primary endpoint of freedom from AF versus 7.3% in the AF drug group (OR, 29.5; CI, 12.0 to 72.2; p<0.001; Figure 1). Seventy-nine percent of patients who were treated with ADT demonstrated chronic treatment failure and crossed over to the cryoablation procedure. In addition, 98.2% of cryoablation-treated patients had acute procedural success; 62.2% of patients were treatment successes without any ADT at 12 months, and 60.1% was considered successful after a single procedure [Packer D. ACC 2010]. Cryoablation patients experienced clinically significant improvements in both the physical and mental components of quality of life areas, measured by the SF-36 questionnaire. In the cryoablation group, there were no atrioesophageal fistulas, 1 patient suffered a stroke that was related to the procedure/device, 3.1% of patients had a pulmonary vein stenosis, and 11.2% (including drug crossovers) had phrenic nerve palsy.

Effectiveness Results: Freedom from AF After 90 Days.
Reproduced with permission from R. Mitrani, MD.
The final technique that was discussed was visually-guided laser, which may achieve success rates that are similar to or superior to radiofrequency ablation and cryoablation. Successful long-term pulmonary vein isolation is reported to be as high as 90%, which is superior to the current technology. After a single procedure, 60% of patients are free from AF.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.