

Summary
This article reports on 10-year survival in 134 myocardial infarction patients who were seen in their medical center between April 1997 and December 1999. The purpose of this retrospective study was to determine length and predictors of survival in patients who presented with acute myocardial infarction to a tertiary care hospital in Trinidad.
- Cardiology Clinical Trials
- Prevention & Screening
- Myocardial Infarction
Roy Tilluckdharry, DM, Int. Med., FCCP, FACC, FESC; Sarasvati Bahadursingh; and Andre Jagroop, Dip. Echocardiography, Cross Crossing Medical Centre, San Fernando, Trinidad, reported on 10-year survival in 134 myocardial infarction (MI) patients who were seen in their medical center between April 1997 and December 1999.
The purpose of this retrospective study was to determine length and predictors of survival in patients who presented with acute myocardial infarction (AMI) to a tertiary care hospital in Trinidad. All patients who were admitted to Cross Crossing Medical Centre between April 1997 and December 1999 with a diagnosis of AMI were identified using the hospital admissions and discharge diagnosis database. Demographic, clinical, and laboratory variables were extracted from the hospital case records of patients with confirmed AMI. This retrospective study investigated 10-year survival among MI patients.
One hundred thirty-four MI patients were tracked during the study period—83 with AMI and 51 with a prior history of MI before April 1997. Mean age of MI occurrence was 55.0 years for males and 59.4 years for females, with an ethnic case mix of 114 (85%) East Indians, 12 (9%) Africans, and 8 (6%) of other descent.
Eighty-three patients (61.9%) were hypertensive, and the same number was diabetic. Twenty-five (18.7%) had a history of cigarette smoking, and 58 (43.3%) had dyslipidemia. Ninety-eight (73.1%) had a left ventricular ejection fraction (LVEF) >45%. Twenty-five (18.7%) had an LVEF between 30% and 45%, and 11 patients (8.2%) had an LVEF that was <30%. The number of involved artery vessels was determined by echo segments: 42 patients (31.4%) had one vessel that was involved, while 61 (45.4%) had two. Three patients (2.2%) had no vessel involvement; 28 (2.9%) had three vessels that were involved.
Out of 134 patients, 36% underwent revascularization; aortocoronary bypass surgery (ACBS; 31%); angioplasty (2%); ACBS and angioplasty (3%); and medical therapy only (64%). Five- and 10-year survival rates were highest in the 45 to 54-year age group. Five-year survival was lowest in the 65 to 74-year age group (56%) and increased to 66.7% in the 75 to 84-year age group. Ten-year survival declined sharply between the 45 to 54-year age group (82.5%) and the 55 to 64-year age group (41.9%; Table 1).
Survival by Age Group after AMI.
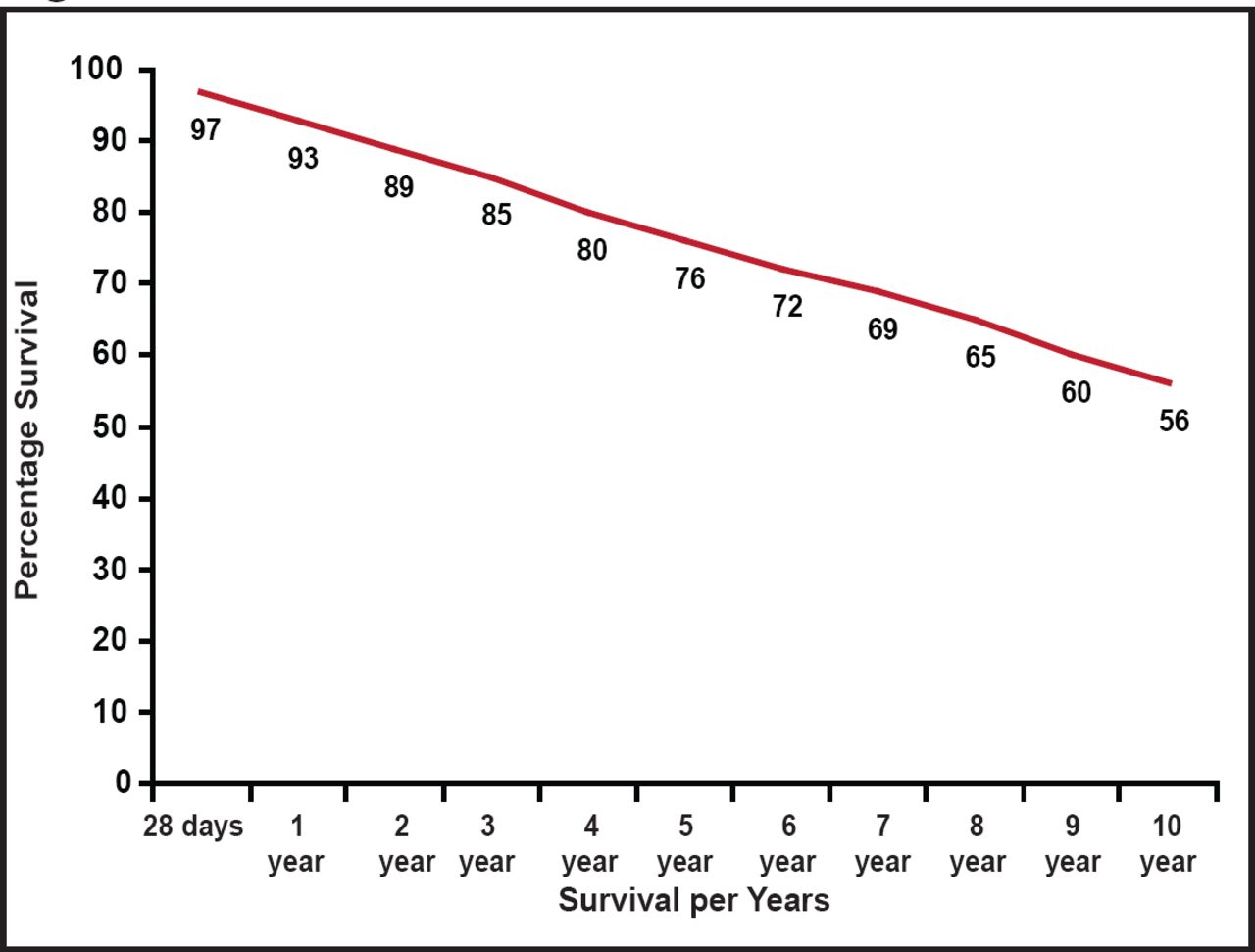
Survival at 5 years was 76%; at 10 years, it was 56% (Figure 1). The researchers found that the main risk factors for mortality were diabetes mellitus (diabetics died 7 to 10 years before their nondiabetic peers), hypertension, and dyslipidemia. MI at a younger age was associated with greater 5- and 10-year survival. Females had higher mortality after MI than males.
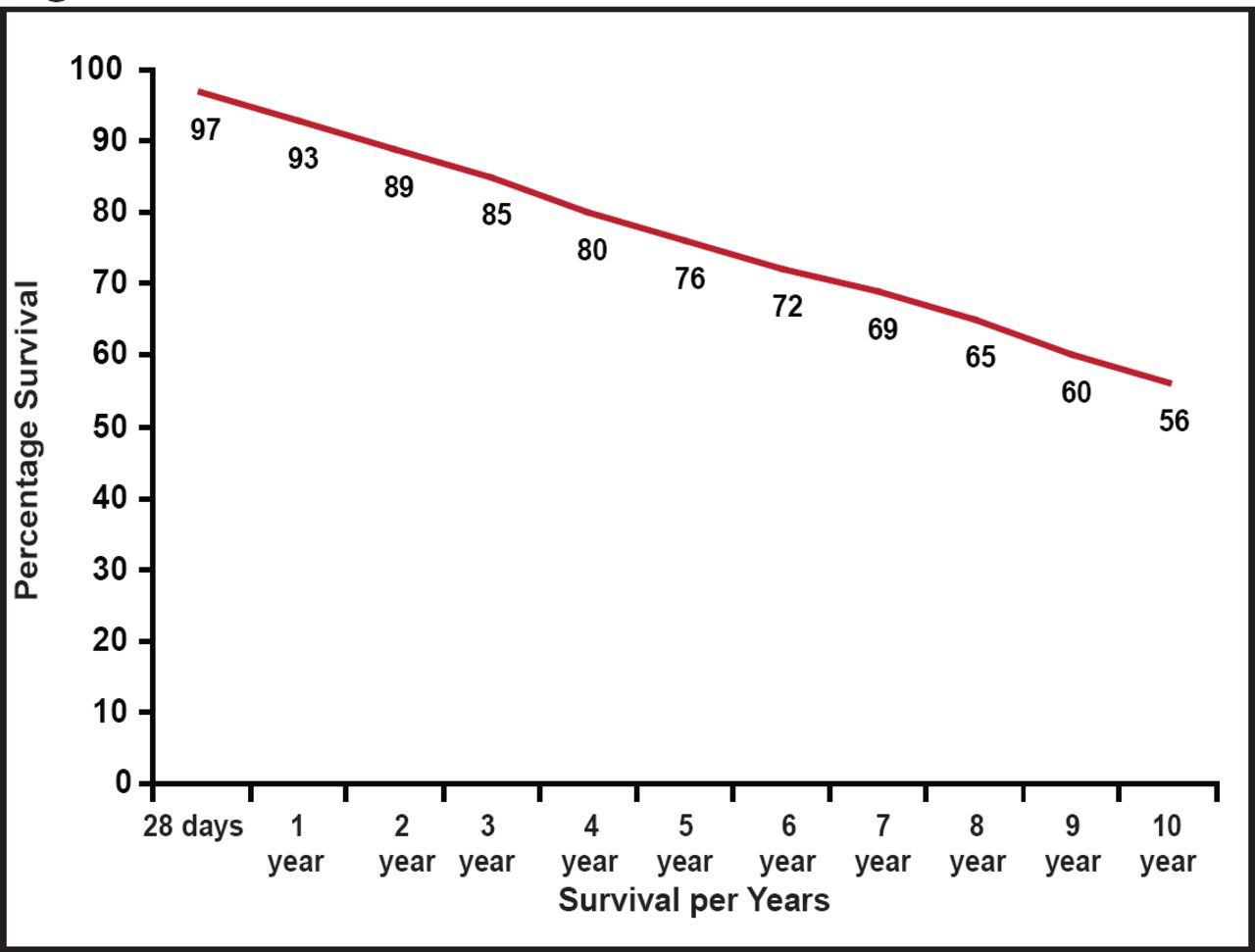
Overall Survival After AMI in Trinidad.
Reproduced with permission from R. Tilluckdharry, DM, Int. Med., FCCP, FACC, FESC.
An epidemiological study of AMI in Tobago found that the most common comorbidities that were associated with AMI were dyslipidemia, hypertension, and diabetes mellitus, followed by end-stage renal disease, smoking, and cocaine use [Alfred R et al. West Indian Med J 2009].
Another report investigated 2-year mortality and its predictors after AMI in Trinidad and Tobago. Three independent predictors of mortality were identified: male sex (p=0.04), in-hospital ventricular fibrillation (p=0.001), and an EF <40% (p=0.02). Diabetes mellitus, hypertension, hyperlipidemia, and cigarette smoking were prevalent among patients who presented with AMI. Ventricular function was a major determinant of 2-year mortality. The authors recommended aggressive risk factor modification to prevent first and recurrent coronary events [Thomas CN et al. West Indian Med J 2000].
Connect with the Caribbean Cardiac Society and MD Conference Express on Facebook!
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.