

Summary
Despite proven efficacy and relatively low cost, key secondary prevention medications are widely underused in populations with prevalent cardiovascular disease particularly in poor countries and rural areas, according to findings from the Prospective Urban Rural Epidemiological [PURE] study.
- Cardiology Clinical Trials
- Prevention & Screening
Despite proven efficacy and relatively low cost, key secondary prevention medications are widely underused in populations with prevalent cardiovascular disease (CVD), particularly in poor countries and rural areas, according to findings from the Prospective Urban Rural Epidemiological (PURE) study.
PURE is the first prospective study to evaluate the use of cardiovascular (CV) drugs for secondary prevention across countries with differing levels of economic development. Salim Yusuf, MD, McMaster University, Hamilton, Ontario, Canada, presented results from the PURE study.
From 2003 to 2009, the PURE study enrolled 153,996 adults from 628 urban and rural communities in 17 countries, with a subset of 5650 patients who reported a prior coronary heart disease (CHD) event and 2292 who reported a prior stroke. Participating countries were classified as high-income (Canada, Sweden, and United Arab Emirates), upper-middle-income (Argentina, Brazil, Chile, Malaysia, Poland, South Africa, and Turkey), lower-middle-income (China, Colombia, and Iran), and low-income (Bangladesh, India, Pakistan, and Zimbabwe), based on World Bank criteria at the beginning of the study. Medical history and use of key secondary preventive medications were assessed with a combination of telephone interviews, home visits, and clinic visits.
Across all countries, only a minority of patients aged 35 to 70 years with a history of CHD or stroke reported taking key secondary preventive drugs, including antiplatelet drugs, aspirin (25.3%), angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs; 19.5%), β-blockers (17.4%), or statins (14.6%).
Between-country variations in medication use were twice as large as patient-level variability due to age, sex, education, smoking, obesity, hypertension, and diabetes, suggesting that national policies and health system structures have a predominant role in secondary prevention.
Medication use was highest in high-income countries and decreased with country income (p-trend <0.0001 for every drug type). Gaps between low-income and high-income countries were approximately 7-fold for aspirin and 20fold for statins. Although 88.8% of patients in high-income countries took at least 1 drug for secondary prevention, far fewer patients received any medication in upper-middle-income countries (54.9%), lower-middle-income countries (30.7%), and low-income countries (19.8%).
There were also differences that were observed between types of communities, with patients in urban areas more likely than those in rural communities to take antiplatelet drugs (28.7% vs 21.3%), β-blockers (23.5% vs 15.6%), ACE inhibitors or ARBs (22.8% vs 15.5%), and statins (19.9% vs 11.6%), regardless of the economic status of the country (p<0.0001 for all drugs). However, gaps between urban and rural medication use were widest in the poorest counties (p interaction<0.0001).
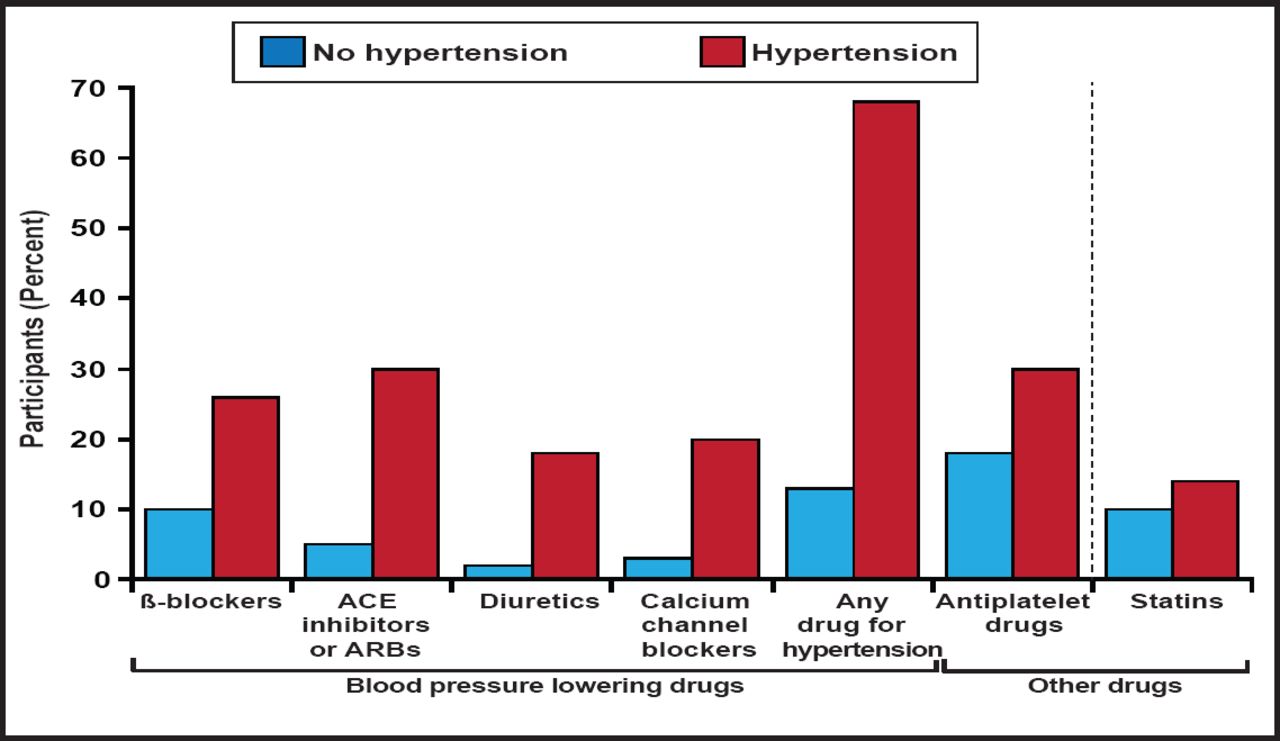
Among patient-level factors, patients with CVD and hypertension were more likely than those with CVD alone to receive drugs that also lowered blood pressure, including β-blockers (28% vs 10%) and ACE inhibitors or ARBs (30% vs 5%; Figure 1). Conversely, younger patients; women; smokers; and those who were less educated, nonobese, or nondiabetic were less likely to use drugs for secondary prevention.

Drug Use by History of Hypertension in Participants with CVD.
Reproduced with permission from The Lancet; Use of secondary prevention drugs for cardiovascular disease in the community in high-income, middle-income, and low-income countries (the PURE Study): a prospective epidemiological survey; Yusuf S et al. 2011.
Long-term follow-up of the PURE study is ongoing. Future reports from the PURE trial will examine specific barriers to effective health care delivery, with the intention of shaping national policies to increase access to medications that are vital for the secondary prevention of CVD.
The results of this large global study underscore the importance of efforts to increase the use of proven secondary preventive therapies and offer an opportunity to reduce CV morbidity and mortality using proven, available, and inexpensive therapies. While the greatest need appears to be in lower-income countries, there appears to be significant underuse in high-income countries as well. These data support the concept of a “polypill,” which has the potential to deliver multiple proven therapies in a single pill in an attempt to close the large treatment gap that was observed in this analysis. The appeal of such an approach is the simplicity that it offers to deliver several drugs at once, which may outweigh the limited flexibility in the selection of the specific drugs and their doses.
- © 2011 MD Conference Express
Additional Reading
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.