

Summary
People who have diabetes are 2 to 4 times more likely to develop cardiovascular disease (CVD) than those without diabetes [World Heart Federation. http://www.world-heart-federation.org/cardiovascular-health/cardiovascular-disease-risk-factors/diabetes/]. This article discusses the importance of diabetes prevention in the prevention of CVD and the efficacy of risk factor modification programs.
- Prevention & Screening
- Diabetes Mellitus
People who have diabetes are 2 to 4 times more likely to develop cardiovascular disease (CVD) than those without diabetes [World Heart Federation. http://www.world-heart-federation.org/cardiovascular-health/cardiovascular-disease-risk-factors/diabetes/].
Jaakko Tuomilehto, MD, MA, PhD, Danube-University Krems, Krems, Austria, discussed the importance of diabetes prevention in the prevention of CVD and the efficacy of risk factor modification programs.
A Powerfully Destructive Duo
The main risk to health in undiagnosed type 2 diabetes mellitus (T2DM) is increased risk of CVD, in particular ischemic heart disease due to coronary atherosclerosis (macrovascular disease) [Waugh N et al. Health Technol Assess 2007]. Impaired glucose tolerance (IGT) is also associated with increased mortality due to ischemic heart disease [Eriksson KF, Lindgarde F. Diabetologia 1998]. Cardiovascular (CV) events account for roughly 80% of deaths among patients with T2DM [Nelson SE. Curr Med Res Opin 2011], and glucose disturbances are twice as common in patients with coronary artery disease as in the general population [Bartnik M et al. Heart 2007].
Prevalence of Diabetes
The prevalence and cost of T2DM are increasing nationwide and globally [Nelson SE. Curr Met Res Opin 2011]. In the past decade in the United States, the incidence of newly diagnosed diabetes in adults has nearly doubled, from a rate of 4.8/1000 in 1997 to 9.1/1000 in 2007 [MMWR Morb Mortal Wkly Rep 2008]. Globally, an estimated 2.8% of the population (171 million people) had diabetes in 2000; this number is expected to rise to 4.4% (366 million people) by 2030 [Wild S et al. Diabetes Care 2004; Nelson SE. Curr Med Res Opin 2011].
Prevention is Key
T2DM is increasingly common, primarily because of increases in the prevalence of sedentary lifestyles and obesity [Tuomilehto J et al. N Engl J Med 2001]. The World Health Organization reports that the most significant modifiable risk factor for T2DM is being overweight or obese [World Heart Federation. http://www.world-heart-federation.org].
The 3-year Finnish Diabetes Prevention Study was one of the first controlled, randomized reports to show that T2DM is preventable with lifestyle intervention [Tuomilehto J et al. N Engl J Med 2001]. The study randomized 522 middle-aged, overweight subjects with impaired glucose tolerance to either a usual care control group or an intensive lifestyle intervention group. The control group received general dietary and exercise advice at baseline and an annual physician's examination. The subjects in the intervention group received additional individualized dietary counseling from a nutritionist. They were also offered circuit-type resistance training sessions and advised to increase their overall physical activity.
Several beneficial changes in clinical and metabolic parameters were observed in the intervention group compared with the control group. Mean weight reduction was 4.2±5.1 kg at Year 1 and 3.5±5.5 kg at Year 3 (p<0.0001) compared with the control group. Significantly greater improvements were seen at Year 1 in fasting plasma glucose (−0.2 vs 0.0 mmol/L), 2-hour plasma glucose (−0.9 vs −0.3 mmol/L), and HbA1C (−0.1 vs 0.1%). During the first 3 years of the study, 22 (9%) in the intervention group and 51 (20%) in the control group developed diabetes (p=0.0001), translating into a 58% relative reduction in the risk of developing diabetes [Tuomilehto J et al. N Engl J Med 2001].
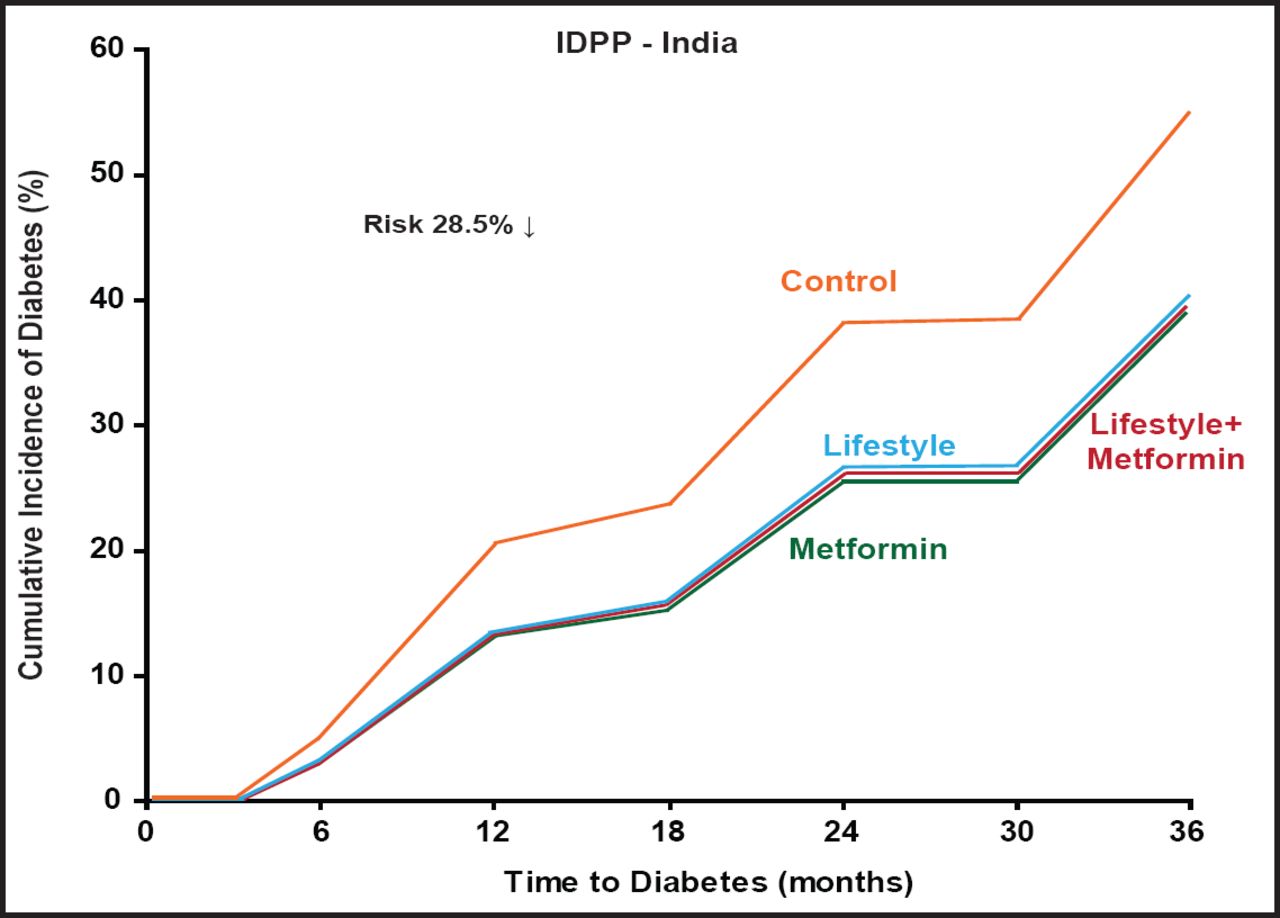
Many other trials have shown that both lifestyle measures and pharmacological treatment can reduce the proportion of people with IGT who would otherwise develop diabetes [Waugh N et al. Health Technol Assess 2007]. In the Diabetes Prevention Program, lifestyle intervention reduced the incidence of diabetes by 58% (95% CI, 48% to 66%) and metformin reduced the incidence of diabetes by 31% (95% CI, 17% to 43%) compared with placebo in patients who were at risk and characterized by elevated fasting and postload plasma glucose concentrations [Knowler WC et al. N Engl J Med 2002]. Using lifestyle interventions, the SLIM trial in the Netherlands showed a 58% decline in risk for diabetes; the EDIPS Newcastle – UK study, 55%; the Da Qing study in China, 43%; and the IDPP study in India, 28.5% (Figure 1).

Prevention of T2DM Through Lifestyle Management.
Springer Verlag. The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1). Ramachandran A et al. Diabetologia; 2006 Feb;49(2):289–97.
Prof. Tuomilehto noted that early intervention in hyperglycemia also has long-term, sustained effects after the end of the intervention. Linstrom et al. [Lindstrom J et al. Lancet 2006] found that beneficial lifestyle changes that were achieved by participants in the intervention group were maintained after the discontinuation of the intervention, and the corresponding incidence rates during the postintervention follow-up were 4.6 and 7.2 (p=0.0401), indicating a 36% reduction in relative risk. Similarly, there was no excess 12-year mortality in men with IGT who participated in diet and exercise in the Malmö Preventive Trial [Eriksson KF, Lindgarde F. Diabetologia 1998].
Screening and Application
Early detection of diabetes could lead to measures to reduce the risk of heart disease [Waugh N et al. Health Technol Assess 2007]. Detection of lesser degrees of glucose intolerance, such as IGT, is worthwhile, in part because the risk of CVD can be reduced with treatment that is aimed at lowering cholesterol levels and blood pressure and in part because some cases of diabetes could be prevented.
The Diabetes Risk Score was developed to identify individuals who are at risk for diabetes without laboratory tests. It was found to be a simple, fast, inexpensive, and reliable tool to identify individuals who are at high risk for diabetes [Lindstrom J, Tuomilehto J. Diabetes Care 2003]. A more recent systematic review and economic modeling study on screening for T2DM found good cause for screening for IGT, with the aim of preventing future diabetes and reducing CVD [Waugh N et al. Health Technol Assess 2007].
The Cardiovascular Health Study evaluated lifestyle risk factors and new-onset diabetes mellitus in older adults and demonstrated that even later in life, combinations of low-risk lifestyle factors are associated with a markedly lower incidence of new-onset diabetes mellitus [Mozaffarian D et al. Arch Intern Med 2009]. Last year, a systematic review of lifestyle modification and glucose intolerance in the prevention of T2DM found that intensive use of nonpharmacological lifestyle interventions, including manipulation of dietary intake and physical activity level, halved the risk of incident diabetes [Thomas GN et al. Curr Diabetes Rev 2010].
The authors concluded that lifestyle modification is a useful weapon in the arsenal for preventing the onset of diabetes. Prof. Tuomilehto agrees: “The prevention of cardiovascular disease in diabetes starts with the prevention of diabetes,” he concluded.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.