

Summary
As many as half of all diabetes patients also have some form of chronic kidney disease (CKD) [www.kidney.org]. A global population of diabetes patients of about 350 million means that there are approximately 150 to 200 million type 2 diabetes patients with CKD'a problem of immense proportions. The combination of diabetes and CKD is characteristic of a specific population of diabetics (eg, those that are older, overweight/obese, hypertensive).
- Diabetes Mellitus
- Renal Disease
- Diabetes & Kidney Disease
As many as half of all diabetes patients also have some form of chronic kidney disease (CKD) [www.kidney.org]. A global population of diabetes patients of about 350 million means that there are approximately 150 to 200 million type 2 diabetes patients with CKD—a problem of immense proportions. Merlin Thomas, MD, Baker IDI Heart and Diabetes Institute, Melbourne, Victoria, Australia, explained that the combination of diabetes and CKD is characteristic of a specific population of diabetics (eg, those that are older, overweight/obese, hypertensive). Although diabetes increases the incidence of a low estimated glomerular filtration rate (eGFR; <60 mL/min), the most common reason for low eGFR is aging, not type 2 diabetes.
Dr. Thomas said he believes that CKD in diabetic patients is mislabeled. Diabetic patients with CKD would be better categorized as having chronic disease, since they are at an increased risk of heart failure, anemia, hypertension, fluid retention, dyslipidemia, malaise/inactivity, treatment side effects, and, in particular, cardiovascular disease (CVD) and premature death. One study that compared the rates of atherosclerotic vascular disease, congestive heart failure, renal replacement therapy, and death in patients with diabetes and/or CKD reported that whereas patients with CKD were at a much greater risk for renal replacement therapy on a relative basis, in absolute terms, the high death rate in this population may reflect accelerated rates of atherosclerotic vascular disease and congestive heart failure (Table 1) [Foley RN et al. JASN 2005].
Adjusted Hazard Ratio by Disease Load.
The effect of CKD in diabetic patients complicates treatment in a variety of ways—in particular, through its effect on glucose control. As eGFR decreases, insulin half-life is prolonged, thus leading to hypoglycemia. In addition, almost one-third of the glucose that is released in response to hypoglycemia comes from the kidney—if the kidneys are not functioning properly, this response is lost. HbA1C is also lower in patients with CKD, even at the same mean glucose control; so, clinicians need to be careful in equating low HbA1C levels in these patients with good glucose control, as this may not necessarily be the case. Finally, CKD is a sign of other pending problems. A patient with an eGFR <60 mL/min/1.73 m2 is at increased risk of a heart attack or stroke and has poorer outcomes from these events, an increased risk of injury-induced fractures, medication-induced adverse events, and poor blood pressure control.
Although the mortality rate that is associated with type 1 diabetes is 5 times higher than that of the general population, it is improving (a decrease of ∼30% over the last 2 decades). In some cases, these improvements exceed gains that are seen in the general population. Presenting data from two large registry studies, Trevor J. Orchard, MD, University of Pittsburgh, Pennsylvania, USA, discussed the factors that are relevant to mortality in patients with type 1 diabetes.
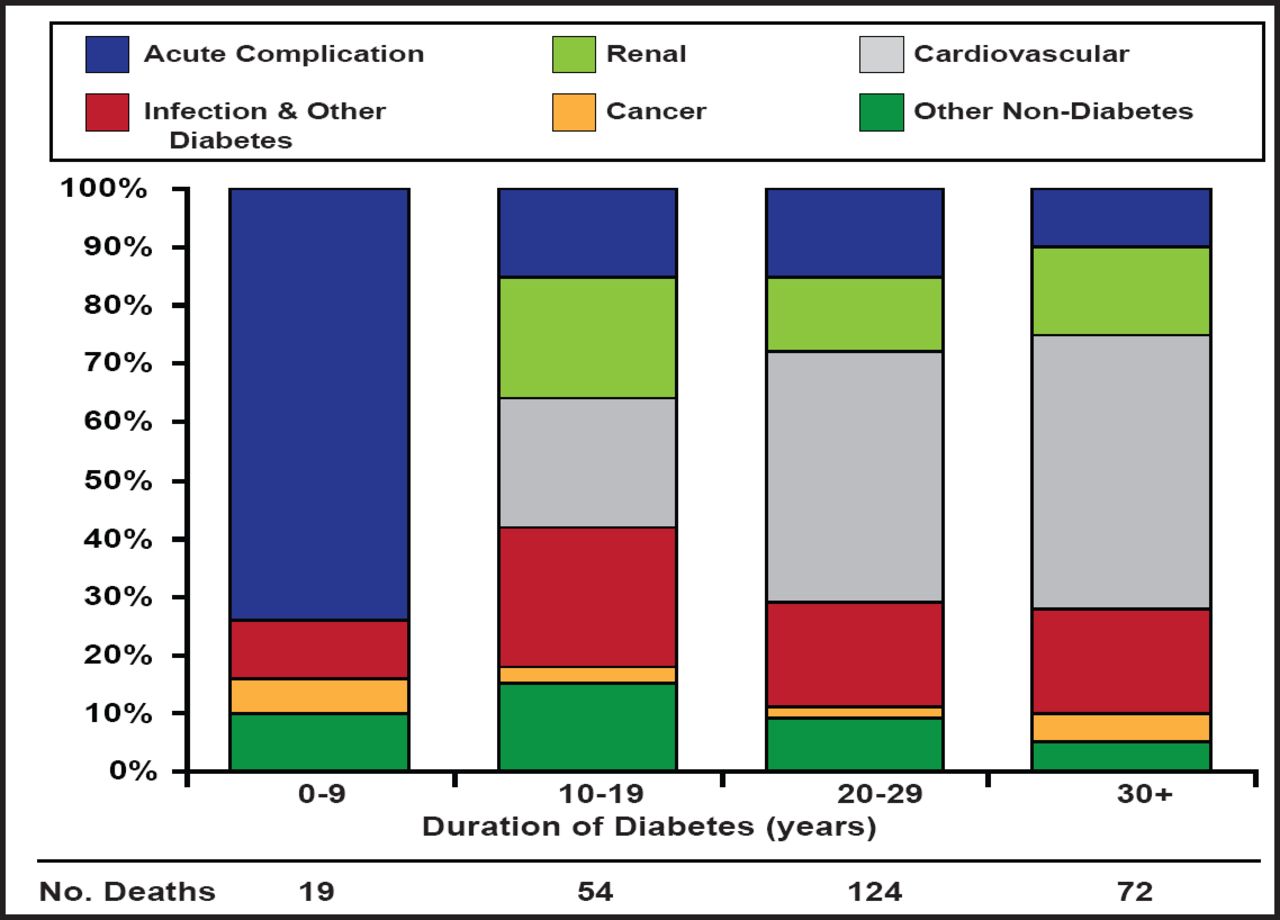
Dr. Orchard discussed the results of a recently published 30-year mortality study from the Allegheny County Type 1 Diabetes Registry, which includes data for 1075 diabetes patients (48% women, 7% black) who were diagnosed between January 1, 1965 and December 31, 1979 [Secrest A et al. Diabetes Care 2010]. The 30-year overall mortality rate was 19% (202 deaths). Mortality rates among blacks were significantly higher than for whites overall and at the 30-year follow-up time point (40.5% vs 17.1%; p<0.001). Thirty-year mortality rates were also higher in women than in men, but the difference was not significant. To determine the trend in mortality over time for patients with diabetes, mortality was analyzed in 3 cohorts, based on year of diagnosis (1965 to 1969, 1970 to 1974, and 1975 to 1979). There was a stepwise decrease in mortality, with the 1965-to-1969 group having significantly higher mortality than the 1975-to-1979 group overall (RR, 1.86: p<0.001) and at 30-years follow-up (RR, 1.51; p=0.02). The study also examined factors that are associated with mortality and found that during the first 10 years of diabetes, acute complications constituted the largest cause of mortality. Renal and CVD were not factors until the second decade, but they predominated thereafter, with renal and CVD contributing to more than 70% of deaths (Figure 1).

Factors Associated with Mortality.
Reproduced with permission from the American Diabetes Association. Cause-Specific Mortality Trends in a Large Population-Based Cohort With Long-Standing Childhood-Onset Type 1 Diabetes. Secrest AM et al. Diabetes Care 2010; 59(12):3216–3222.
The impact of renal disease was also shown in the Finnish Diabetic Nephropathy (FinnDiane) study, a national, multicenter, 7-year follow-up study of 4201 adults with type 1 diabetes that showed a clear association between the presence and severity of CKD and all-cause mortality. At baseline, mean age and duration of diabetes ranged from 36 to 44 years and 20 to 32 years, respectively, depending on renal status. A total of 12% of participants had microalbuminuria, 14% had macroalbuminuria, and 7% had end-stage renal disease (ESRD). Over the 7-year period, there were 291 deaths. Standardized mortality rates were 0.8 for participants with normal albuminuria, 2.8 for those with microalbuminuria, 9.2 for those with macroalbuminuria, and 18.3 for those with ESRD [Groop PH et al. Diabetes 2009].
Dr. Orchard discussed a recent study that further examined cause of death by renal status using data from the Pittsburgh Epidemiology of Diabetes Complications (EDC) Study, which included 658 subjects with childhood-onset type 1 diabetes (age <17 years). Participants in the EDC study had a mean age of 28 years with a mean duration of diabetes of 19 years. Renal disease was defined as an albumin excretion rate ≥20 μg/min from multiple samples and grouped as microalbuminuria (20–200 μg/min), overt nephropathy (>200 μg/min), or ESRD (dialysis or renal transplantation). At baseline, 311 (47.3%) individuals had renal disease (microalbuminuria 21.3%, overt nephropathy 22.2%, and ESRD 3.8%). Over a median follow-up of 20 years, there were 152 deaths (23.1%). Mortality was 6.2 (95% CI, 5.2 to 7.2) times higher than expected. Standardized mortality ratios were 2.0 (1.2 to 2.8) for participants with normoalbuminuria; 6.4 (4.4 to 8.4) for those with microalbuminuria; 12.5 (9.5 to 15.4) in the presence of overt nephropathy; and 29.8 (16.8 to 42.9) for participants with ESRD. Excluding those (n=64) with normoalbuminuria who later progressed to renal disease, there was no excess mortality among the subjects in the remaining normoalbuminuria group (1.2; 0.5 to 1.9), whose deaths were largely unrelated to diabetes. These results support the FinnDiane findings and extend them up to 20 years, showing that type 1 diabetes patients without renal disease can achieve long-term survival that is comparable with the general population [Orchard TJ et al. Diabetologia 2010].
Microalbuminuria not only represents the early stage of diabetic nephropathy but also reflects widespread vascular damage and is a marker of insulin resistance in type 1 diabetes, as well as a predictor of CVD, irrespective of diabetes status. In the HOPE study, the relative risk for major cardiovascular events was 1.97 and 1.61 in those with and without diabetes, respectively [HOPE Study Investigators. N Engl J Med 2000]. Thus, as microalbuminuria is also associated with numerous other risk factors/markers and with general vascular damage, the total concordance between microalbuminuria and the excess mortality of type 1 diabetes probably reflects much more than early renal disease alone.
- © 2011 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.