

Summary
This article discuesses the results of the ADVISE trial, which evaluated instantaneous wave-free ratio, a new technology that assesses coronary stenosis using pressure as a surrogate for coronary flow during a period of naturally occurring stable resistance, thereby avoiding the need for adenosine or other vasodilators.
- Cardiology Clinical Trials
- Coronary Artery Disease
- Valvular Disease
Fractional flow reserve (FFR) is a diagnostic tool that is utilized during coronary angiography to determine the physiological significance of a coronary artery stenosis. FFR is defined as the ratio of the pressure that is distal to a stenosis relative to the pressure before the stenosis during maximal hyperemia. Although FFR has been validated in clinical trials and correlated with improved outcomes, recent evidence has shown that only 6% of percutaneous coronary interventions (PCIs) in the United States are performed with FFR guidance [Kleiman NS et al. J Am Coll Cardiol 2011]. A major barrier to its use is the current requirement for vasodilator drugs, such as adenosine, which may be contraindicated or disliked by patients, and it adds to procedural time and costs, inconvenience, and risk [Pijls N. J Am Coll Cardiol Interv 2011].
Justin Davies, MD, PhD, Imperial College, London, UK, presented the results of the ADVISE trial, which evaluated instantaneous wave-free ratio (iFR), a new technology that assesses coronary stenosis using pressure as a surrogate for coronary flow during a period of naturally occurring stable resistance, thereby avoiding the need for adenosine or other vasodilators.
The first part (proof-of-concept) of the ADVISE study evaluated resting wave-free resistance versus mean hyperemic resistance in 39 patients. Study assessments included intracoronary pressure and flow velocity measurements, baseline resistance assessment, and resistance assessment under pharmacological vasodilatation. The investigators found that resistance that was measured at rest during the wave-free period was similar in both stability (p=0.96) and magnitude (p=0.70) to values that were achieved under adenosine hyperemia.
The second part of the study evaluated whether the assessment of the significance of a coronary stenosis was numerically similar using iFR and FFR in 157 patients. iFR is defined as an instantaneous pressure ratio across a stenosis during the wave-free period, when resistance is constant and minimized in the cardiac cycle. The FFR was measured following administration of intravenous adenosine to achieve maximal hyperemia.
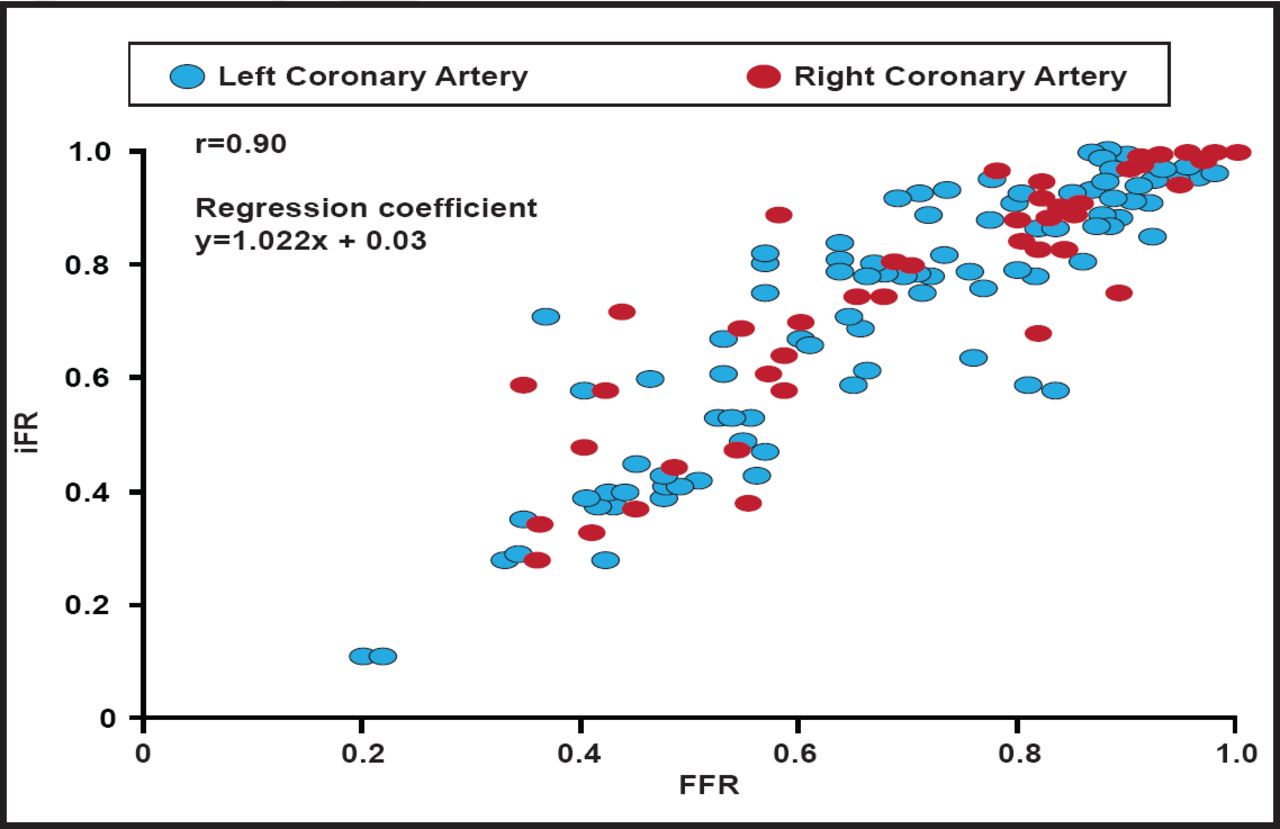
Measurement of iFR during the wave-free period provided a measure of stenosis severity that was similar to the FFR measurement (r=0.90, regression coefficient y=1.022x + 0.03; Figure 1). The small difference between iFR and FFR was not explained by the magnitude of hyperemia (Figure 2).

Close relationship between iFR and FFR.
Reproduced with permission from J. Davies, MD, PhD.

Magnitude of Hyperemia.
Reproduced with permission from J. Davies, MD, PhD.
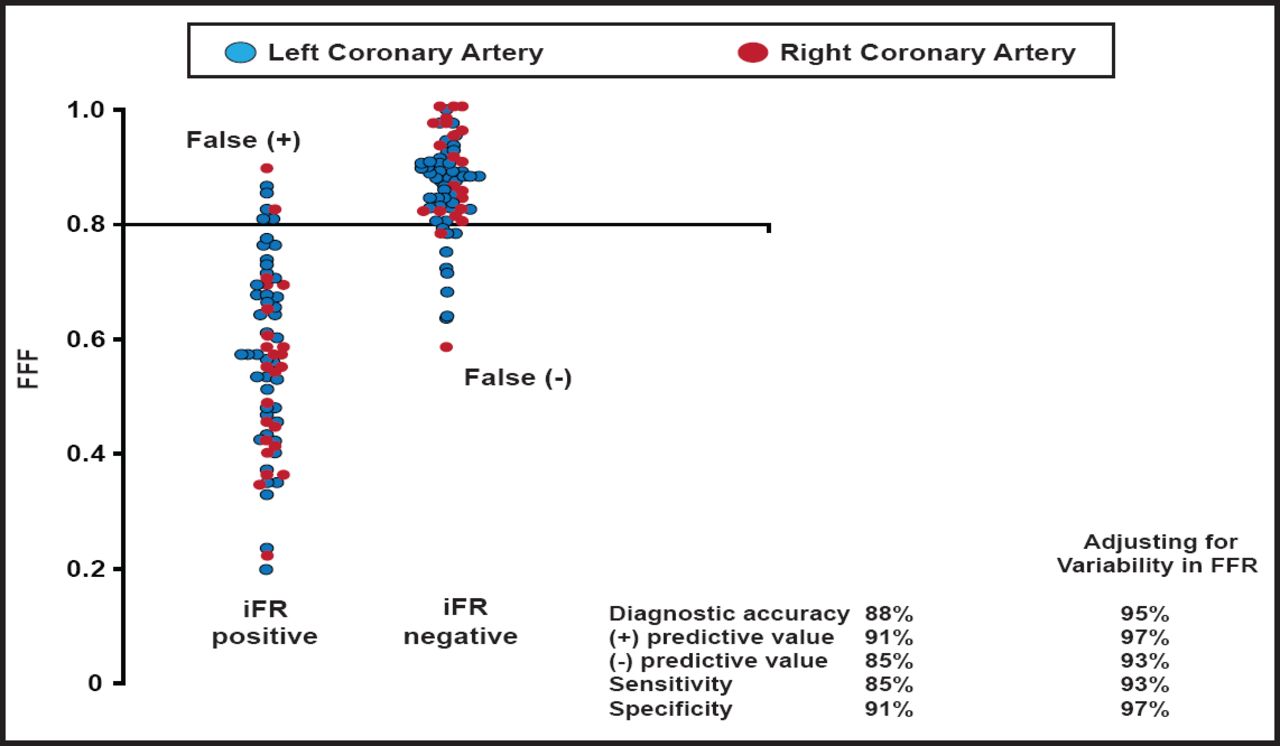
Assessment of the diagnostic efficiency of iFR demonstrated a diagnostic accuracy of 88%, positive predictive value of 91%, negative predictive value of 85%, sensitivity of 85%, and specificity of 91%. After adjustment for the inherent variability in FFR, diagnostic accuracy was 95%, positive predictive value was 97%, negative predictive value was 93%, sensitivity was 93%, and specificity was 97% (Figure 3).

Assessment of Diagnostic Efficiency of iFR After Adjustment for Inherent Variability in FFR.
Reproduced with permission from J. Davies, MD, PhD.
The ADVISE study identified a wave-free period in the cardiac cycle when resistance is naturally stabilized and minimal, obviating the need for administration of adenosine. iFR that is measured during this wave-free period gives a measure of stenosis severity that is similar to that provided by FFR. The clinical implications of these results include removal of barriers to adoption of physiological assessment, increased applicability, improved work flow in the catheter laboratory, and improved patient experience.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.