

Summary
The Endovascular Valve Edge-to-edge Repair Study [EVEREST II; NCT00209274] compared the percutaneous implantation of a clip that grasps and approximates the edges of the mitral leaflets at the origin of the regurgitant jet with conventional surgery for mitral value repair. Percutaneous repair, however, is less effective at reducing mitral regurgitation than conventional surgery. However, the procedure was associated with better safety and improvements in other secondary outcomes, such as left ventricular dimensions and New York Heart Association class [Feldman T et al. N Engl J Med 2011].
- Valvular Disease
- Interventional Techniques & Devices
The Endovascular Valve Edge-to-edge Repair Study (EVEREST II) compared the percutaneous implantation of a clip that grasps and approximates the edges of the mitral leaflets at the origin of the regurgitant jet with conventional surgery for mitral value repair [NCT00209274]. Laura Mauri, MD, Brigham and Women's Hospital, Boston, Massachusetts, USA, concluded that percutaneous repair was less effective at reducing mitral regurgitation (MR) than conventional surgery. However, the procedure was associated with better safety and improvements in other secondary outcomes, such as left ventricular dimensions and New York Heart Association (NYHA) class [Feldman T et al. N Engl J Med 2011].
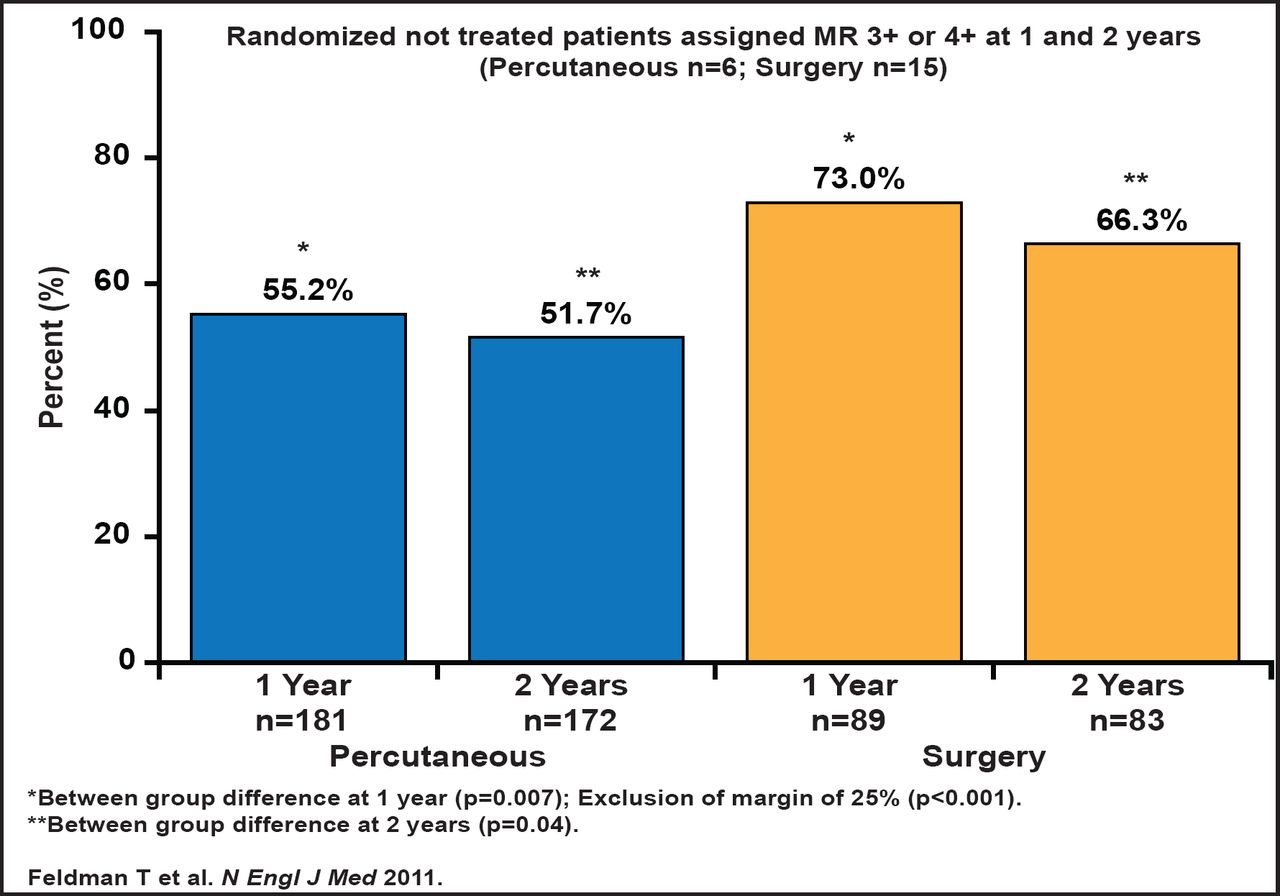
Patients with moderately severe or severe (grade 3+ or 4+) MR were randomly assigned in a 2:1 ratio to undergo either percutaneous repair (n=172) or conventional surgery (repair or replacement; n=83). The primary composite endpoint for efficacy was freedom from death, surgery for mitral valve dysfunction, and grade 3+ or 4+ MR at 1 year. The primary safety endpoint was a composite of major adverse events (MAE) within 30 days. The 1- and 2-year rates of the primary endpoint for efficacy were 55% and 52%, respectively, in the percutaneous repair group and 73% and 66% in the surgery group (p=0.007 at Year 1 and p=0.04 at Year 2; Figure 1).

Primary Effectiveness Analysis at 1 and 2 Years (ITT Population).
Reproduced with permission from L. Mauri, MD.
The differences were driven largely by a need for surgery for mitral valve dysfunction in the percutaneous repair group (20% vs 2%; p<0.001 at 12 months; 22% vs 4%; p<0.001 at 2 years). At 2 years, mortality was similar (∼11% in each group, p=NS). Grade 3+ or 4+ MR rates for the two treatments were similar. For the percutaneous arm, 2+ MR was more common, while 1+ was more common for surgery (p<0.05). Left ventricular volume improved for both groups and was maintained through the 2-year follow-up; however, there was a significant difference that favored surgery. NYHA functional class improved from baseline in both groups at both 1 and 2 years, with a more favorable outcome in the percutaneous group, with less frequent occurrence of NYHA Class II and IV (p<0.05 for difference at both years).
Quality of life was assessed using the SF-36. The percutaneous group showed improvement at 30 days and at 12 months on both the physical (3.1±9.4 and 4.4±9.8) and mental components (4.4±11.3 and 5.7±9.9; all p<0.001). There was a slight, early (at 30 days) decline in the physical component for the surgery group (−4.9±13.3; p=0.004), with a late improvement (12 months) on the mental component (3.8±10.3; p=0.006).
While the overall results favored surgery, exploratory subgroup analyses showed that patients aged <70 years, those with degenerative MR, and those with a left ventricular ejection fraction (LVEF) >60% had better outcomes with surgery. Meanwhile, patients aged ≥70 years, those with functional MR, and those with LVEF <60% had similar outcomes between the two procedures. MAEs occurred in 15% of patients in the percutaneous repair group and 48% of patients in the surgery group at 30 days (p<0.001). More transfusions due to bleeding occurred in the surgery group. Dr. Mauri noted that the difference in the safety endpoint was driven by bleeding. Future trials will directly evaluate the subset of patients who are at high surgical risk or have left ventricular dysfunction.
Nimesh D. Desai, MD, Hospital of the University of Pennsylvania, Philadelphia, Philadelphia, USA, discussed the latest innovations in the transfemoral transaortic valvular implantation (TAVI) treatment of severe aortic stenosis in high-risk patients; these recent innovations may allow for the safer use of these devices to treat a larger, lower-risk subset of patients. The current generation of TAVR devices is still prone to having difficulty with access and can be faulted for lack of control and accuracy in positioning/placement of the valve, and valves can not be fully resheathed or retrieved if necessary and are subject to paravalvular leaks, conduction disturbances that require a permanent pacemaker, and cerebral embolization. New technology exists to address almost all of these issues. Dr. Desai recommends the Paieon system, as it provides for excellent valve positioning and postemployment measurements, and the St. Jude Portico™ TAVI system, which is a first-in-human resheathable device. Stroke has always been a major issue with TAVI, and the Embrella® Embolic deflector is a new device that has the potential to reduce the risk of cerebral embolism and stroke. Once deployed, a porous membrane shields the brachiocephalic trunk and the left carotid artery, deflecting emboli away from the cerebral circulation [Nietlispach F et al. J Am Coll Cardiol Intv 2010]. The key to the successful use of these new devices is cooperation between surgeons and cardiologists.

The editors would like to thank the many members of the AHA Scientific Sessions 2011 presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2011 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.