

Summary
Interventional strategies have evolved over the past decade, and determining an optimal approach depends on many factors. This article discusses the latest developments in cardiac intervention.
- interventional techniques & devices
Interventional strategies have evolved over the past decade, and determining an optimal approach depends on many factors. Samin Sharma, MD, FACC, Mt. Sinai Medical Center, New York, NY, discussed the latest developments in cardiac intervention.
Left ventricular assist device (LVAD) support may be indicated for high-risk percutaneous coronary intervention (PCI) cases in the presence of severe left ventricular (LV) dysfunction (ejection fraction [EF] <30%), complex lesions in which transient closure may be catastrophic, large myocardial infarction (MI) with hemodynamic instability, or cardiogenic shock. The ongoing PROTECT II trial is evaluating the Impella Recover 2.5 system compared with a traditional intra-aorta balloon pump (IABP) during high-risk elective PCI procedures. A total of 654 elderly patients with triple vessel disease (mean age 69 years and mean EF 26.1±6%) will be randomized as part of this prospective, multicenter trial. The Impella system is a miniaturized LVAD system that is placed percutaneously via the femoral artery and actively unloads the ventricle, providing up to 2.5 L/min of flow with support up to 5 days. This device decreases myocardial O2 demand and thus augments coronary and end-organ perfusion. The primary outcome is the composite rate of intraprocedural and postprocedural major events, including death, MI, stroke, transient ischemic attack, target vessel revascularization, coronary artery bypass grafting (CABG), acute renal failure, and severe hypotension [Sharma S. TCT 2009]. Secondary outcomes include maximum cardiac power output decrease from baseline and the rate of in-hospital major cardiac events (MACE) for Impella compared with IABP. Thus far, the rate of successful implantation for the Impella system is 100%, with 80% freedom from 1-year MACE for the first 20 consecutive elderly patients. Of these 20 patients, 40% required rotational atherectomy (n=8). Further results for the PROTECT II trial are pending.
The Coronary Sinus Reducer Stent, a percutaneous implantable device that is designed to narrow the coronary sinus and elevate coronary sinus pressure, may be a future option for patients with refractory angina who are not good candidates for conventional revascularization procedures. The first-in-man study of 15 patients showed that the Coronary Sinus Reducer Stent is safe and feasible for the treatment of refractory angina when conventional revascularization is not an option [Banai S et al. J Am Coll Cardiol 2007]. Larger studies are required to further establish these findings.
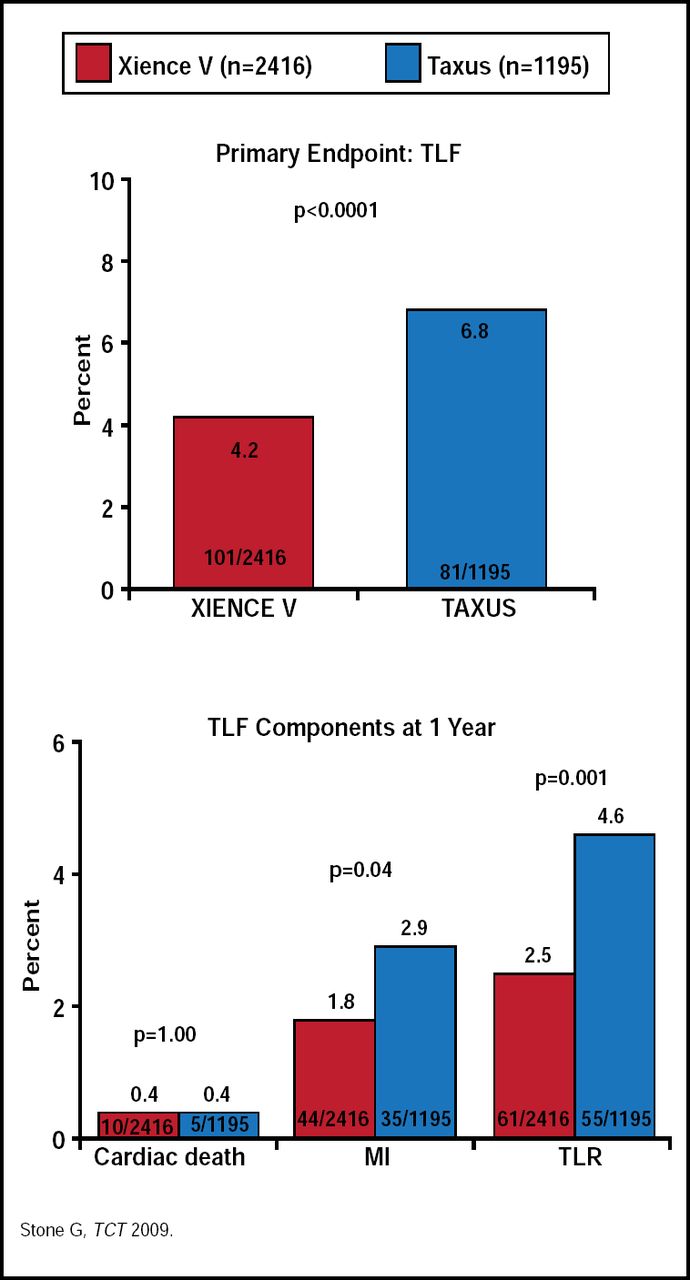
Drug-eluting stents (DES) have also evolved, and we are now seeing many studies that are comparing first-and second-generation DES. Stone and colleagues are comparing everolimus-eluting (EES) with paclitaxeleluting stents (PES) in the ongoing SPIRIT IV trial [Stone G. TCT 2009]. In this study, 3690 patients with a maximum of 3 lesions in 3 separate coronary arteries were randomized (2 to 1) to receive either EES or PES, after which they received aspirin ≥80 mg for 5 years and clopidogrel ≥75 mg for at least 12 months (when not at risk for bleeding). Clinical follow-up occurred at 1, 6, and 9 months and annually for 1 to 5 years.
The primary endpoint was target lesion failure (TLF), defined as the composite of cardiac death, target vessel MI, or ischemia-driven target lesion revascularization. There was a significant reduction in TLF that was associated with the EES compared with the PES (38% RRR; p<0.0001) at 1 year (Figure 1). Additionally, there was an 80% hazard reduction (95% CI, 27% to 94%; p=0.002) in stent thrombosis in the EES group compared with the PES group. There was no significant difference between the two groups for TLF in patients with diabetes [Stone G. TCT 2009]. Five-year outcomes are pending.

SPIRIT IV: One-Year Clinical Results.
Bioabsorbable stent technology is also at the forefront of interventional cardiology. Preliminary findings from the ABSORB study showed that at 2 years postimplantation, vasomotion (ie, normal vasodilation and vasoconstriction) had been restored at the stented site and adjacent coronary artery and restenosis had been prevented in patients who received bioabsorbable EES. Of the 30 patients who were included in this pilot study, there was one non-Q wave MI but no cardiac death, ischemia-driven target lesion revascularization, or stent thrombosis that was recorded [Serruys PW et al. Lancet 2009]. The next arm of this study is underway and includes 80 patients.
Thrombus aspiration is another effective interventional technique. In the Thrombus Aspiration during Percutaneous Coronary Intervention in Acute Myocardial Infarction Study (TAPAS), investigating 1071 patients with possible ST-segment elevation MI, Svilaas and colleagues found that thrombus aspiration during PCI resulted in better reperfusion and clinical outcomes than conventional PCI. The thrombus aspiration group showed complete resolution of ST-segment elevation in 56.6% of patients and a myocardial blush grade of 0 to 1 in 17.1% of patients compared with 44.2% and 26.3% in the conventional PCI group, respectively (p<0.001 for both) [Svilaas T et al. N Engl J Med 2008].
There are many new innovations in the area of interventional cardiology. Advancements are being made with the development of new technologies and approaches. It is important to remain visionary and continue in the pursuit of optimal therapies. Over the next decade, we will see the development of new areas of interventional therapy with a focus on safety and simplicity, concluded Dr. Sharma.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.