

Summary
The concept that the clinical successes that are seen in individual patients can and must be replicated and scaled up to a population level if we are ever to have a world that is free of diabetes and its complications.
- Diabetes Mellitus
- Prevention & Screening
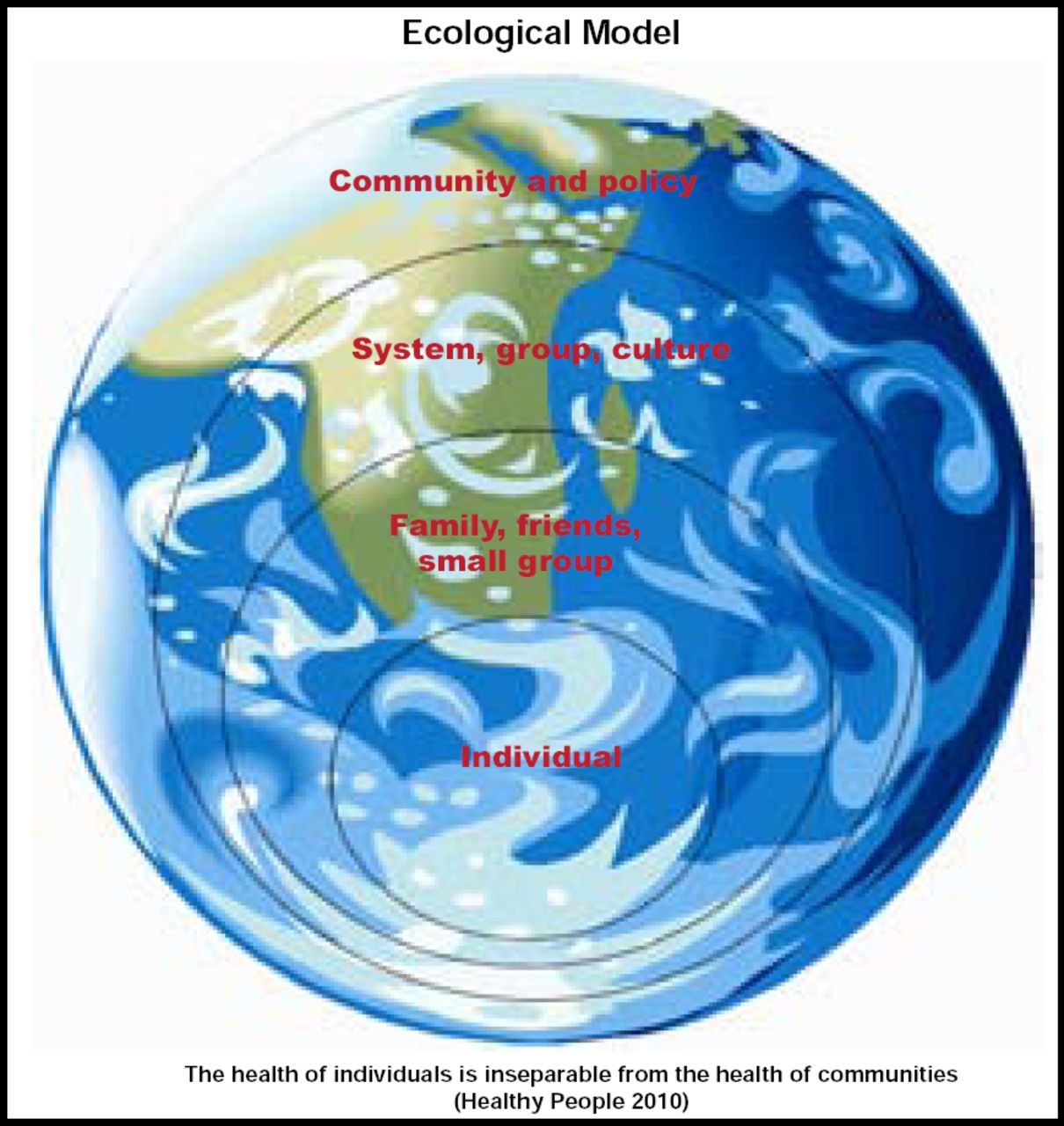
The concept that the clinical successes that are seen in individual patients can and must be replicated and scaled up to a population level if we are ever to have a world that is free of diabetes and its complications was the subject of the State-of-the-Art Lecture at the 70th Scientific Sessions of the American Diabetes Association. Ann Albright, PhD, RD, Director, Division of Diabetes Translation, Centers for Disease Control, Atlanta, GA, represented this concept using an ecological model, visually represented by an image of concentric circles—the individual at the center, surrounded by extended family and friends, encircled by the culture, and encapsulated by the community (Figure 1). Dr. Albright encouraged policymakers and public health professionals, as well as health care providers, to be mindful of the importance of achieving population goals without losing sight of the individual. “The health of individuals is inseparable from the health of communities and societies,” she said.
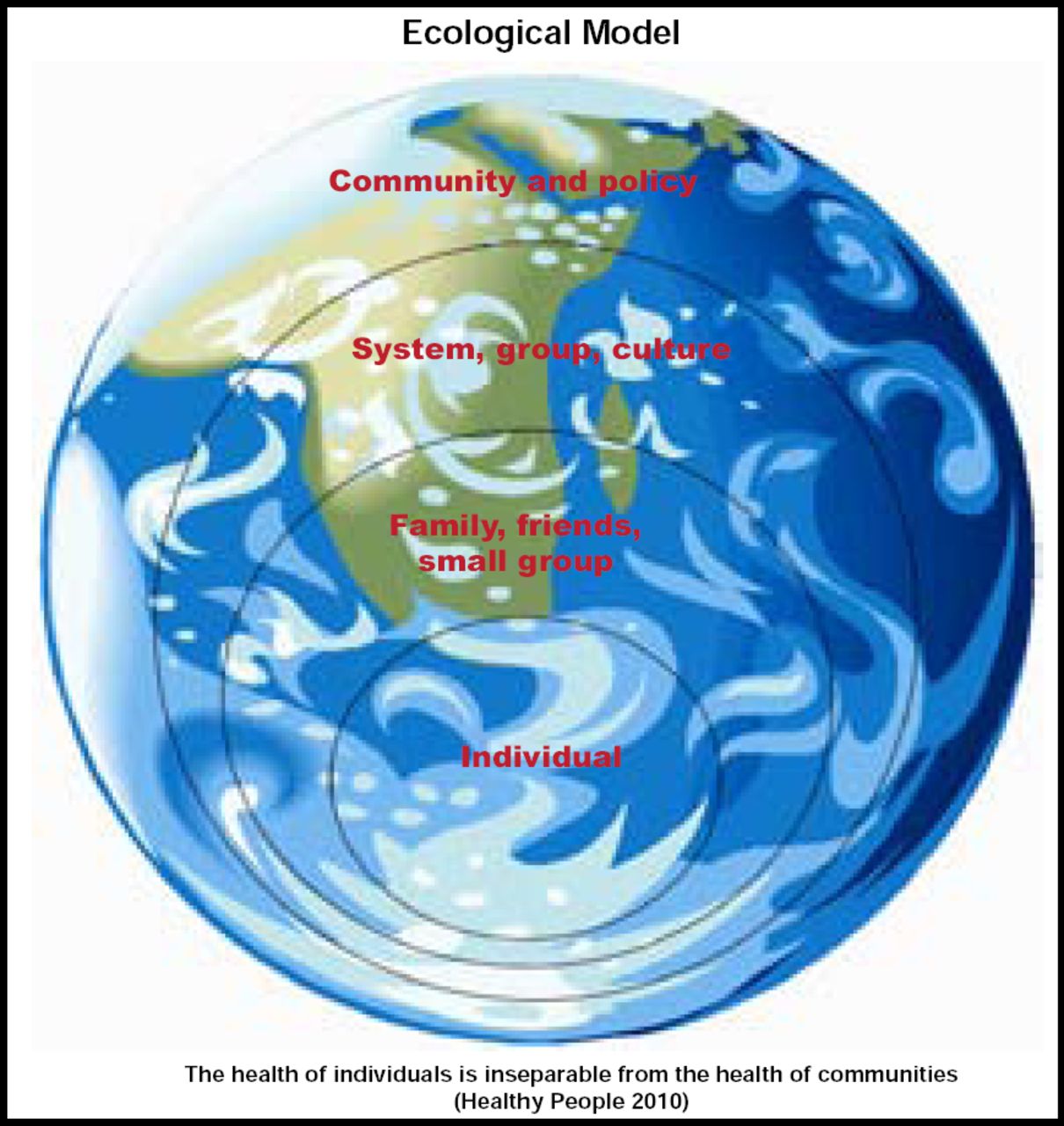
Ecological Model.
Reproduced with permission from A. Albright, PhD.
As a result of improved medications and devices, advances in self-management, and community-based training, there have been improvements in diabetes care on an individual level. Data from 1995–2005 show that advances in care have brought about decreasing rates in some comorbidities that are associated with diabetes. Vision loss has decreased 25%; foot ulcers and amputations are down 36%; kidney failure has declined by 23%; and cardiovascular disease hospitalizations are down 16% [www.cdc.gov/diabetes]. Despite this progress, population-based measurements show that care for many subpopulations of Americans with diabetes still falls short. It is estimated that 2 in 5 people with diabetes still have poor lipid control, 1 in 3 have poorly controlled blood pressure, and 1 in 5 have not achieved glycemic control [Saaddine et al. Ann Intern Med 2006].
The number of people with diabetes continues to grow. Data from 1997–2003 indicate that the incidence (new cases) of diabetes has increased from 4.9 to 6.9 per 1000 population (p<0.01), and the prevalence of obesity between 1997–1998 and 2002–2003 has risen from 14.2 to 18.3 per 1000 population (p=0.02) [Geiss LS et al. Am J Prev Med 2006]. Increasing life expectancy, earlier diagnosis, and fewer people going undiagnosed account for some of the increased prevalence of diabetes, but the increase in new cases of diabetes is the major contributor. Unfortunately, the gains that are being made in diabetes control are being overwhelmed by the increased incidence. Continued advances for those with the disease, as well as for those who have yet to develop it, are needed. Wise choices should be made about programs and public policies that will have the greatest impact and can be achieved and sustained on a large scale, if we are truly going to make inroads in reducing the incidence and, ultimately, the prevalence of diabetes.
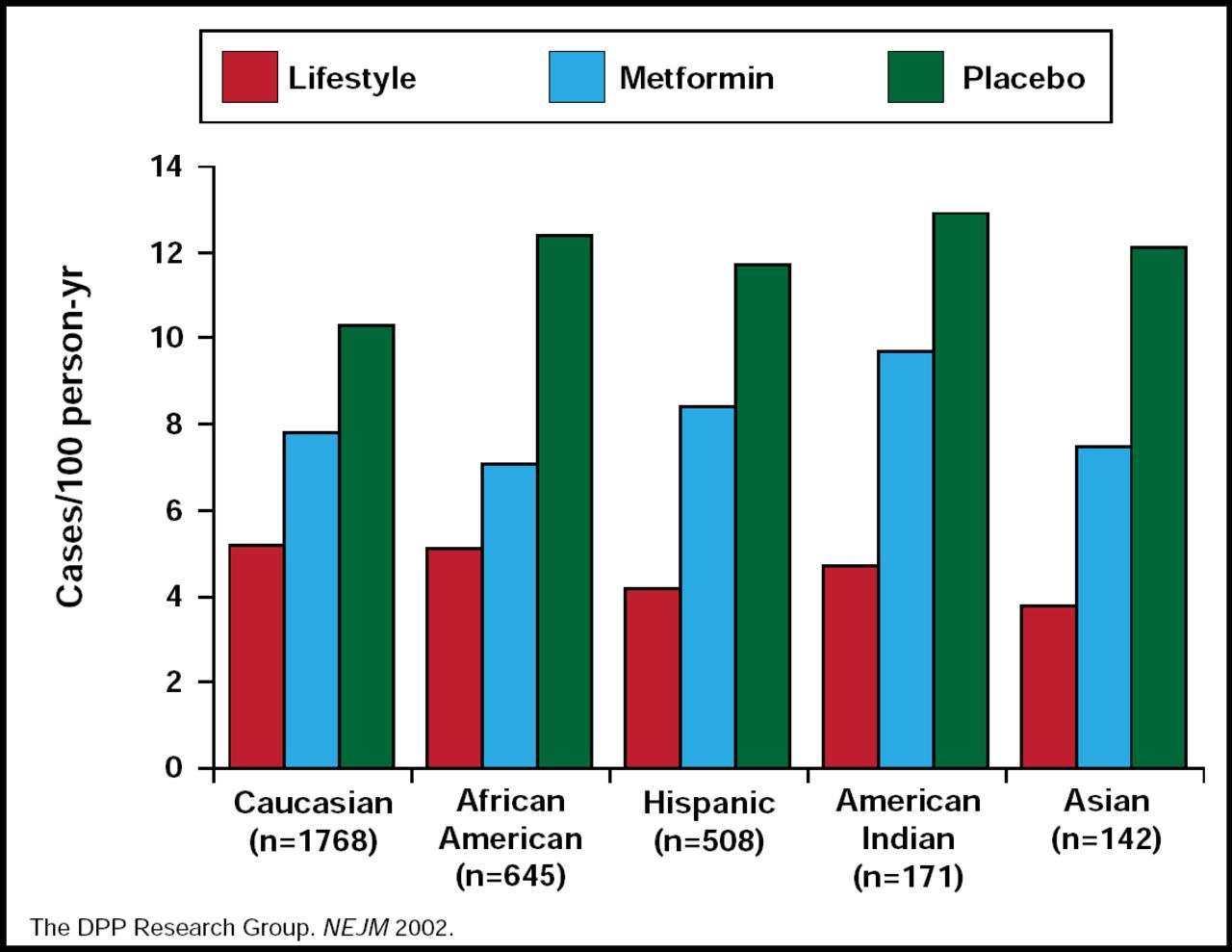
The landmark Diabetes Prevention Program (DPP) showed that a 58% (95% CI, 48 to 68) reduction in the incidence of type 2 diabetes can be achieved in those with prediabetes through a structured lifestyle intervention that achieves 5% to 7% weight loss through low-fat/low-calorie food choices and 150 minutes of physical activity a week [The DPP Research Group. N Engl J Med 2002]. The improved outcome was demonstrated in all racial and ethnic groups that were studied (Figure 2).
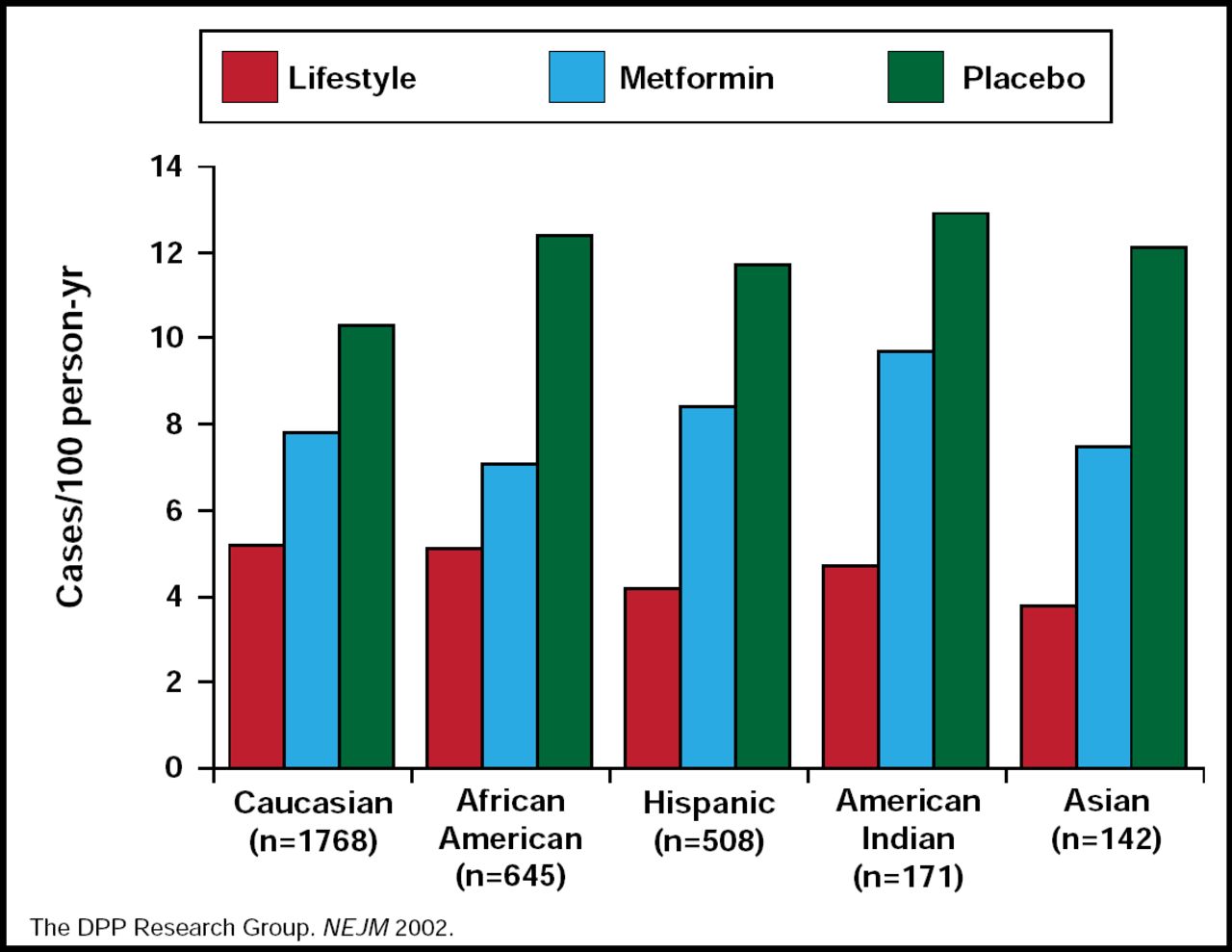
DPP Study: Intervention Impact by Ethnicity.
Reproduced with permission from A. Albright, PhD.
Subsequent translation studies that have shown that the DPP intervention can be successfully and cost-effectively delivered in community-based group settings have demonstrated that these findings can be implemented on a large scale to achieve a population impact. As a result, the National Diabetes Prevention Program was initiated. Its mission is to systematically scale the translated model of the DPP for high-risk people, performed in collaboration with community-based organizations, health payers, public health, academia, and others to reduce the incidence of type 2 diabetes in the United States.
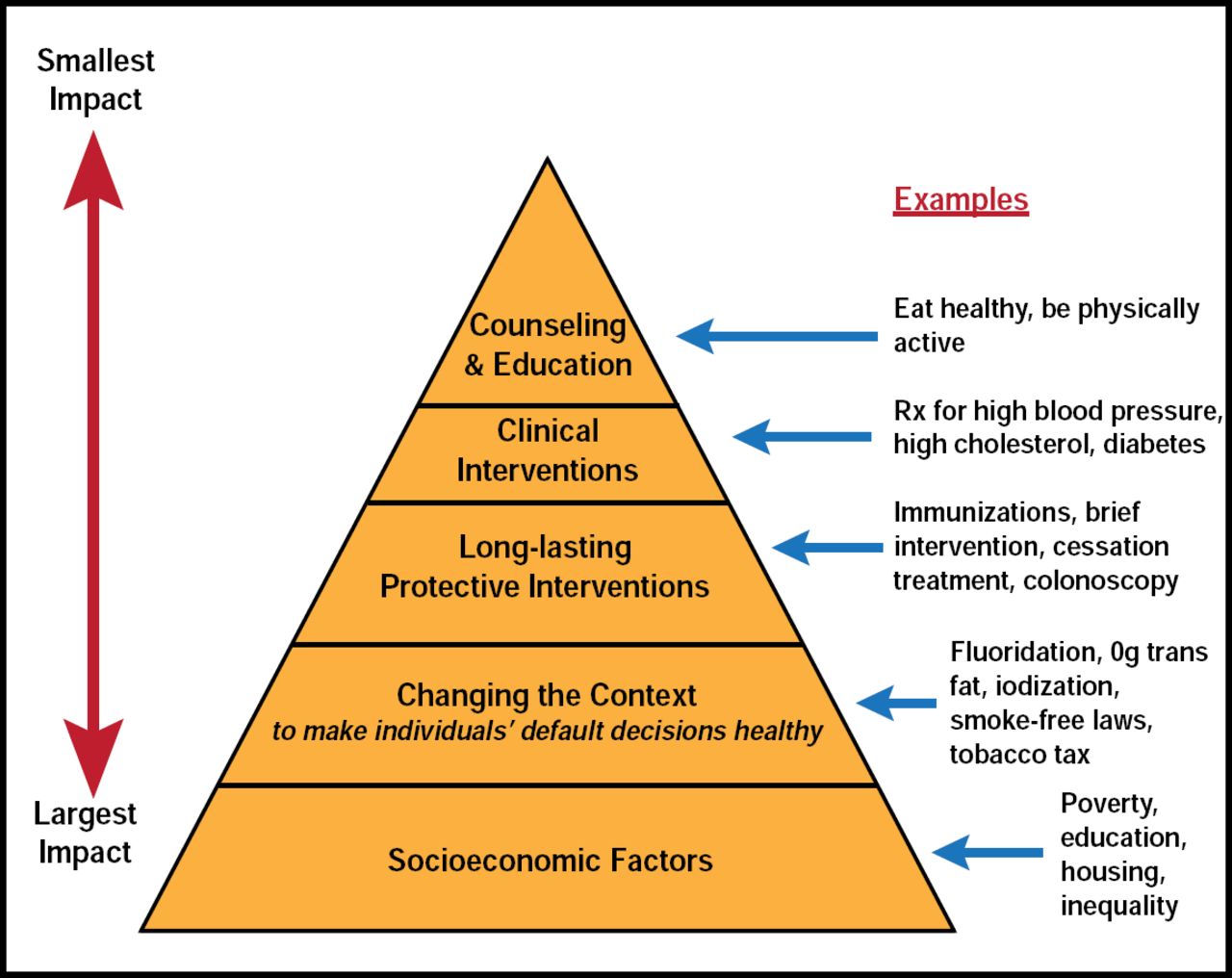
To illustrate the complexity of factors that affect health, Dr. Albright used the health impact pyramid, developed by Dr. Thomas Frieden, Director of CDC (Figure 3). At the pinnacle, where the structure is most narrow in scope (and societal impact), are individual counseling and education. Supporting the pinnacle are clinical interventions (medications); below that, and broader in scope, are long-term interventions—single-touch, lasting effects. Near the bottom of the pyramid are the even broader initiatives that change the population's health-related context and make healthy choices the default choices. Underpinning the entire structure and having the greatest impact are socioeconomic factors, such as poverty, education, and housing. Without change at the bottom, stated Dr. Albright, gains at the top will be difficult to achieve. It is important to note that all elements in the pyramid are important and necessary.
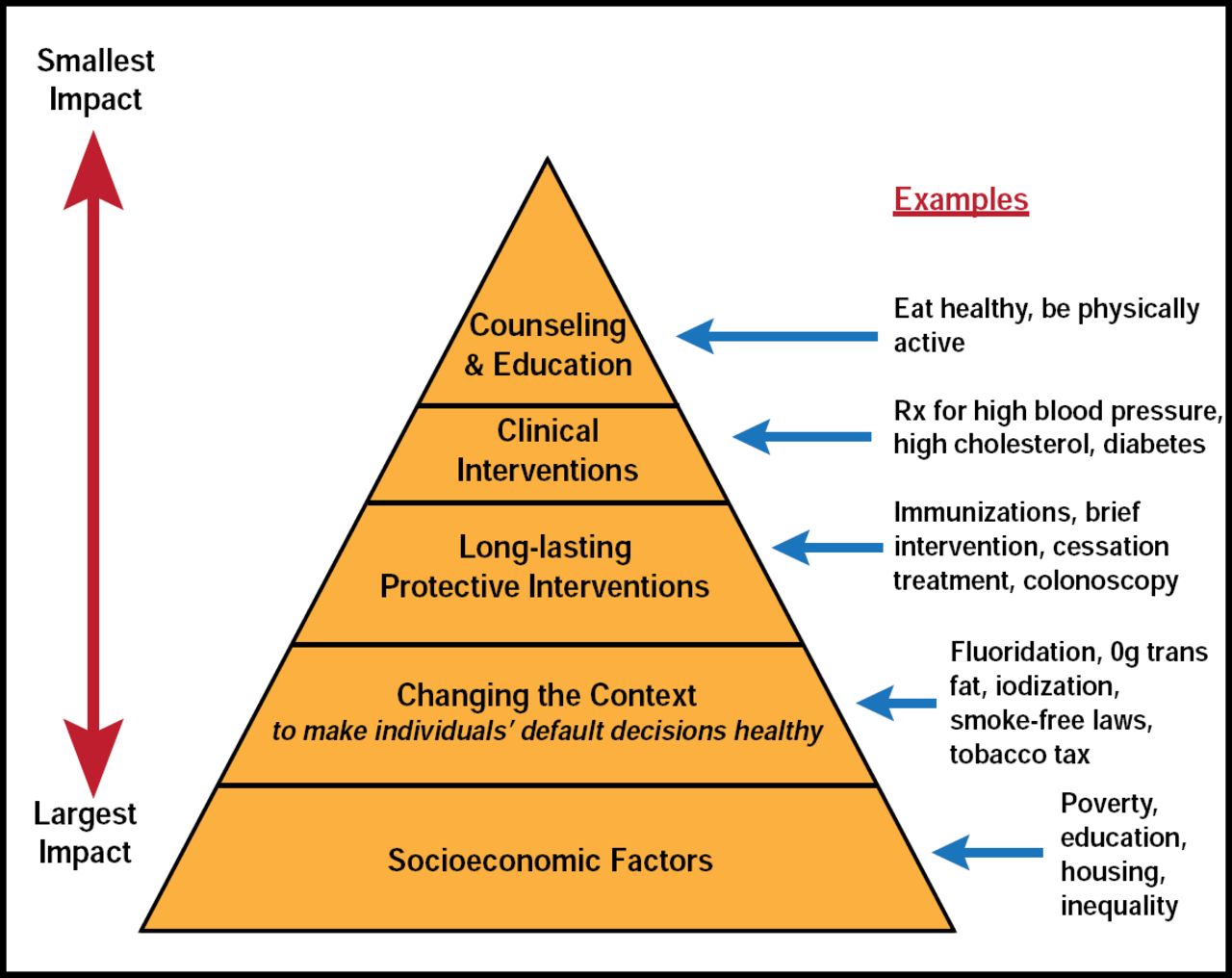
Factors that Affect Health.
Reproduced with permission from A. Albright, PhD.
In practical terms, implementing programs that will bring about change will require a partnership between practitioners and the community. For diabetes prevention, these programs provide opportunities for clinicians to have short interactions with patients about their risk. The individual would then be referred to a community-based organization that is prepared and equipped, and is being reimbursed to deliver the necessary intervention services. While some sample groups are implementing this procedure, more community-based organizations and payers are needed to deliver the interventions and provide the reach and scalability that are required for a population-based effect.
“In order to achieve the goal of a world free from the devastation of diabetes, we need to work at an individual level but also the population level to have a large-enough impact to achieve this critical goal,” Dr. Albright concluded.
- © 2010 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.