

Summary
Subarachnoid hemorrhages that result from ruptured aneurysms initiate a series of events that may result in very poor outcomes. This article give an overview of the biological mechanisms of vasospasms that result from ruptured aneurysm blood clots.
- ischemia
- interventional techniques & devices
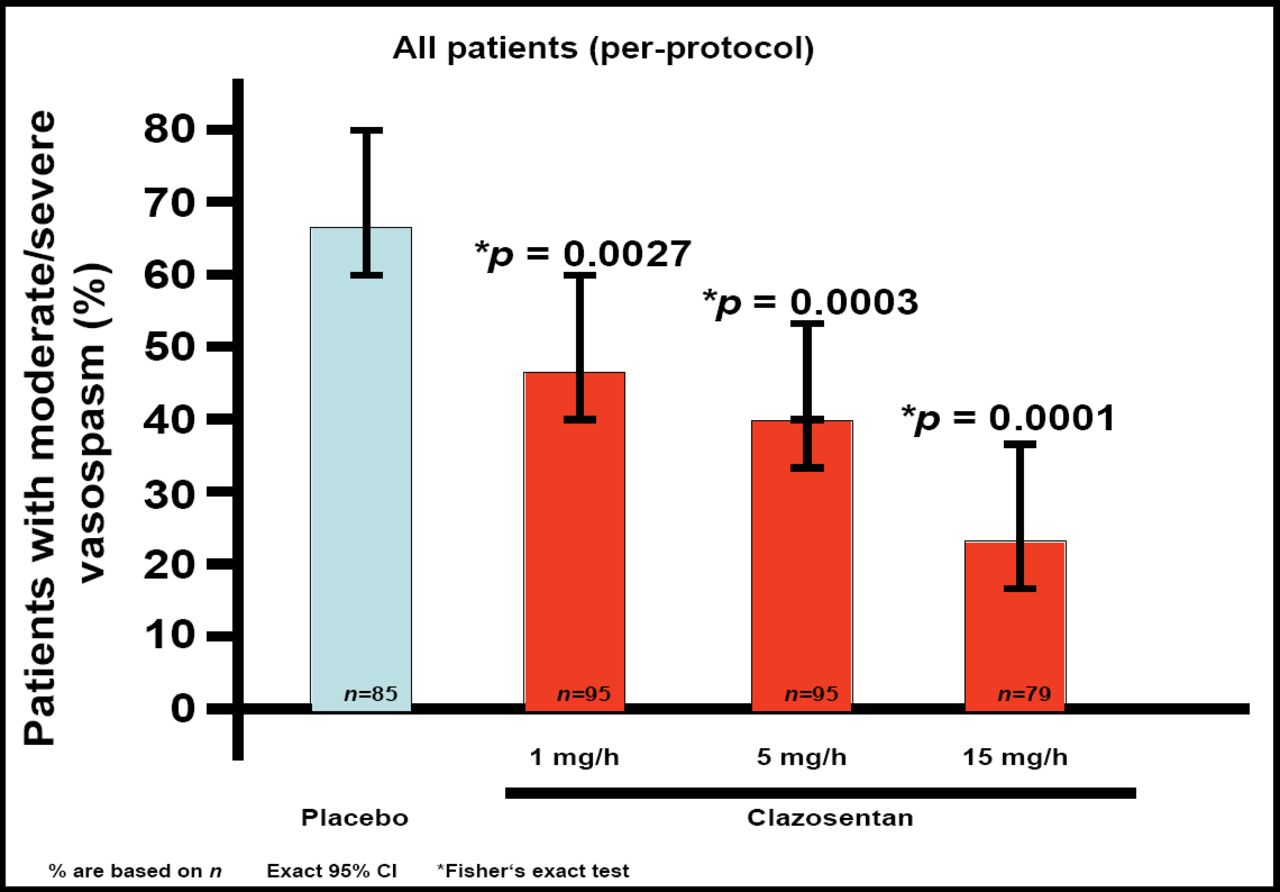
Subarachnoid hemorrhages that result from ruptured aneurysms initiate a series of events that may result in very poor outcomes. R. Loch MacDonald, MD, University of Toronto, Toronto, Ontario, Canada, gave an overview of the biological mechanisms of vasospasms that result from ruptured aneurysm blood clots. “The erythrocyte seems to be the component of the blood that is primarily responsible for initiating the delayed angiographic response that occurs,” said Dr. MacDonald. The vasospasms are related to smooth muscle contraction, possibly due to increases in endothelin or prostaglandins, decreases in the relaxant nitric oxide, neurotransmitters, membrane depolarization, increased sensitivity to calcium, or impairment of muscle relaxation pathways. Barth et al (Stroke 2007) conducted a study of the calcium channel blocker nicardipine in 32 patients undergoing craniotomy for aneurysm. Nicardipine pellets (40 mg) were placed in the basal cisterns of 16 patients. On Day 8, the incidence of vasospasms in the nicardipine-treated patients was reduced from 73% to 7% (p<0.05) and mortality between treated (6%) and placebo patients (38%) reached statistical significance (p=0.042). “This fits with the depolarization mechanism of vasospasm,” noted Dr. MacDonald. In preclinical models, endothelin antagonists are successful in preventing vasospasm. This was confirmed in the phase 2 CONSCIOUS-1 study. Three doses of clazosentan were used to treat patients with subarachnoid hemorrhage, and all 3 doses were significantly better than placebo in preventing vasospasm (Figure 1). In addition to the effects of the blood clot, secondary processes such as disturbance of the blood brain barrier, hypertension, brain edema, apoptosis, and global ischemia are at play. “It starts to become even more complicated when you add in these other mechanisms…all can contribute to ischemia, infarction, and poor outcome,” said Dr. MacDonald.

Clazosentan Prevents Cerebral Vasospasm.
Given the serious consequences of vasospasm, researchers have proposed performing angioplasty as prophylactic treatment. Richard Latchaw, MD, University of California, Davis, CA, presented work from Jonathan Hartman, MD, Kaiser Permanente Sacramento Medical Center, Sacramento, CA, that explored this approach. “This is a dangerous procedure…every time I do angioplasty on a post-subarachnoid hemorrhage patient, I really respect those vessels because they are very tender vessels. It's very easy to produce overdilitation and rupture,” cautioned Dr. Latchaw. The Balloon Prophylaxis of Aneurysmal Vasospasm (BPAV) study was a phase 2 trial that was conducted to determine if prophylactic angioplasty performed within 96 hours of a Fisher grade III or III+IV subarachnoid hemorrhage would alleviate vasospasm. The study enrolled 170 patients and was conducted at 10 centers in the US, Canada, and the Netherlands. Based on 3 deaths that occurred during the study, the protocol was modified to exclude A1 and P1 segments, as it was believed that these were too dangerous. A total of 81 patients received prophylactic angioplasty, with 1 perforation and 3 deaths. There was no statistically significant difference between the group that received balloon angioplasty and the control group in terms of vasospasm, outcomes at 3 months, length of hospital stay, or the probability of delayed ischemic neurological deficits. “One of the confounding factors is that the ballooned patients tended to have a higher degree of hydrocephalus, which may have made that group look a little worse,” noted Dr. Latchaw. However, the need for therapeutic balloon angioplasty was significantly higher in the control group (p=0.03). “This is the most significant part of this study,” concluded Dr. Latchaw.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.