

Summary
The precise relative risk of stroke in pregnancy is not currently known, and the occurrence of stroke has dire consequences for both mother and fetus. According to the 2005 National Health Interview Survey, 253,000 women aged 18–44 years reported that they had been told by a clinician that they had suffered a stroke [Pleis et al. Vital Health Stat 2007]. This article discusses the risk of stroke and its relationship to ovarian hormones throughout the lifespan.
- hormone therapy
- pregnancy
- cerebrovascular disease
- prevention & screening
The precise relative risk of stroke in pregnancy is not currently known, and the occurrence of stroke has dire consequences for both mother and fetus. According to the 2005 National Health Interview Survey, 253,000 women aged 18–44 years reported that they had been told by a clinician that they had suffered a stroke (Pleis et al. Vital Health Stat 2007). The risk of stroke and its relationship to ovarian hormones throughout the lifespan was the subject of the Ovarian Hormones, Pregnancy and Stroke: Risks, Management and Prevention symposium. Steven J. Kittner, MD, MPH, University of Maryland, College Park, MD, reviewed best management practices for expectant mothers who had suffered a previous non-cardioembolic stroke. Current guidelines state that the appropriate treatment for a pregnant woman with non-cardioembolic stroke is unfractionated heparin (UFH) or low molecular weight heparin (LMWH) for the first trimester, followed by low-dose aspirin during the second and third trimesters (Sacco et al. Stroke 2006). Antithrombotic therapies and their associated Food and Drug Administration (FDA) pregnancy ratings are listed below.
FDA Antithrombotic Therapy Pregnancy Ratings.
Dr. Kittner pointed out that FDA pregnancy ratings must be interpreted carefully, as not all ratings are based on equivalent data. “Clopidogrel's B rating was based only on data that described no evidence of risk in animals; human data were not available. With low molecular weight heparin, there is no evidence of risk in either animal or human data,” commented Dr. Kittner.
Preeclampsia is characterized by new onset hypertension (systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg) combined with new onset proteinuria (>300 mg/24 hours). The prevalence and outcomes of preeclampsia were summarized by Cheryl Bushnell, MD, MHS, Wake Forest University, Winston-Salem, NC. The pathophysiology of preeclampsia is thought to be related to an abnormal constriction of the uterine spiral artery, although the exact mechanism remains unknown. Preeclampsia occurs in approximately 5% of pregnancies, with 75% of episodes occurring in the last 4 weeks of pregnancy. The presenting neurologic symptoms of severe preeclamspia are headache, confusion, visual deficits, hyperreflexiaor clonus, and hemiparesis. Primary risk factors for preeclampsia include a family history of preeclampsia, prior pregnancy with preeclampsia, chronic hypertension, obesity, and diabetes. Dr. Bushnell believes that the growing number of women with obesity, diabetes, and hypertension will lead to a future increase in preeclampsia. “It's important to remember that preeclampsia is one of the major causes of maternal mortality [15–20%], and of the women who die from preeclampsia, 40% die from cerebrovascular complications. It's very important to understand the implications of having had a stroke related to preeclampsia,” emphasized Dr. Bushnell.
The serious consequences of preeclampsia affect both fetus and mother. Fetal complications include early delivery, growth restriction, hypoxia-associated neurologic injury, perinatal death, and long-term cardiovascular effects associated with low birthweight (Sibai et al. Lancet 2005). Mothers may experience vasculopathy, pulmonary edema, abruptio placentae, disseminated intravascular coagulation, HELLP syndrome, hemorrhagic stroke, and ischemic stroke. The risk of a peripartum stroke is 4 times higher if a woman experiences preeclampsia. These strokes are most likely to be post-partum and related to very high blood pressure.
Mothers with preeclampsia are being followed to determine the long-term consequences of this condition. Wilson et al (BMJ 2003) found that these women are twice as likely to develop cerebrovascular disease. In another study, Ray et al (Lancet 2005) found that women with a history of maternal placental syndromes were twice as likely to develop cardiovascular disease. Given the risks, complications, and morbidity of preeclampsia, it is not surprising that physicians need tools to identify this condition as early as possible. A study by Levine et al (NEJM 2006) found that preeclampsia was preceded by increased levels of soluble endoglin 2–3 months prior to onset (10.2 ng/mL in preeclampsia vs 5.8 ng/mL in controls; p<0.001). The authors also found that increased soluble fms-like tyrosine kinase:placental growth factor ratios paralleled the rise of endoglin, with women in the upper quartile for both biomarkers having the highest risk of developing preeclampsia. “This type of research is really advancing the field of preeclampsia and its detection,” said Dr. Bushnell.
The risks and benefits of hormone replacement therapy (HRT) have been the subject of much debate and discussion in recent years. The incidence of stroke in women is relatively low until after menopause, and observational studies implied that HRT patients were protected from stroke and cardiovascular disease. Additionally, preclinical studies indicated that estrogen was neuroprotective. Louise McCullough, MD, University of Connecticut, Farmington, CT, reviewed the historical data and what this information means for stroke prevention in older women today.
Although HRT appeared to have great promise in women's health, data from large-scale trials in post-menopausal women failed to demonstrate clear benefits. The Heart and Estrogen/Progestin Replacement Study (HERS) trial (Hulley et al. JAMA 1998) enrolled 2763 post-menopausal women with coronary disease and an intact uterus. This study found no reduction in cardiac endpoints or stroke in HRT patients. In the Women's Estrogen and Stroke (WEST) trial, 664 women were randomized to estrogen or placebo. The HRT group had an increased rate of stroke and death from stroke. Additionally, if a woman had a stroke, it was more severe if she was on HRT (Viscoli et al. NEJM 2001). The Women's Health Initiative HRT study enrolled 16,608 healthy post-menopausal women. Women received estrogen plus progestin, and the data indicated an increased risk of ischemic stroke in the HRT group. This increased risk was present regardless of age, presence of hypertension, or history of cardiovascular disease (Rossouw et al. JAMA 2002). As of today, “there is no role for estrogen replacement therapy or hormone replacement therapy as it is currently prescribed for stroke prevention either in women with established vascular disease or for primary prevention,” said Dr. McCullough.
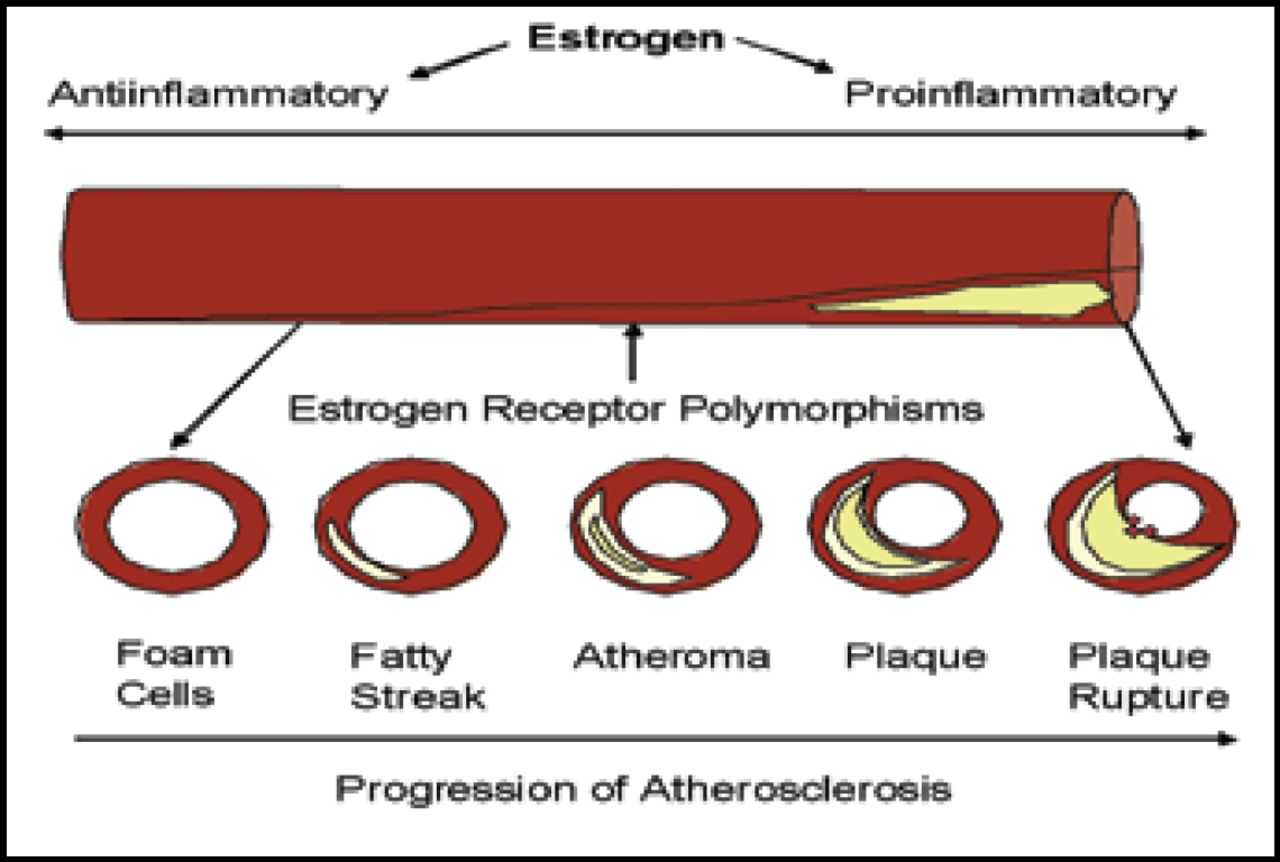
What this means is that the timing of HRT, the best types of patients for HRT, and the relative risks of HRT still need to be defined. It is possible that estrogen has a proinflammatory effect in vessels that have already deteriorated and that the protective benefit may exist only before damage to the vasculature occurs (Figure 1). For this reason, new trials are underway to further the understanding of HRT and its role in women's health. The Kronos Early Estrogen Prevention Study (KEEPS) trial is an ongoing randomized, controlled multicenter trial of HRT in women who recently went through menopause. Participants will receive either oral or transdermal estrogen with intermittent micronized progesterone and will be followed for 5 years (Kuo et al. Lancet 2005). Studies such as the KEEPS trial should provide additional guidance that will hopefully translate into improved stroke prevention for women.

Chronology of the Development of Atherosclerosis.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.