

Summary
The advantage of prasugrel over clopidogrel in preventing stent thrombosis has been found to be maintained regardless of the time since the stenting procedure, the type of stent, or the ARC definition of thrombosis. The TRITON-TIMI 38 stent analysis showed that the drug led to a highly significant reduction in stent thrombosis over a broad array of clinical and procedural characteristics.
- interventional techniques & devices
- myocardial infarction clinical trials
- thrombotic disorders
The advantage of prasugrel over clopidogrel in preventing stent thrombosis has been found to be maintained regardless of the time since the stenting procedure, the type of stent, or the ARC definition of thrombosis. The TRITON-TIMI 38 stent analysis showed that the drug led to a highly significant reduction in stent thrombosis over a broad array of clinical and procedural characteristics.
The patients who were included in the stent analysis represented a subset of patients from the main TRITON-TIMI 38 trial, which included patients with moderate-to-high-risk acute coronary syndrome who were scheduled for PCI. In that trial, 6461 patients received only bare-metal stents (BMS), and 5743 patients received only drug-eluting stents (DES). The patients were randomly assigned to antiplatelet therapy with either clopidogrel (300 mg loading dose before PCI, followed by a maintenance dose of 75 mg daily for one year) or prasugrel (loading dose of 60 mg, followed by 10 mg daily for one year). The findings of that study showed that prasugrel was associated with a 52% reduction in stent thrombosis (2.4% compared with 1.1% for clopidogrel; p<0.0001).
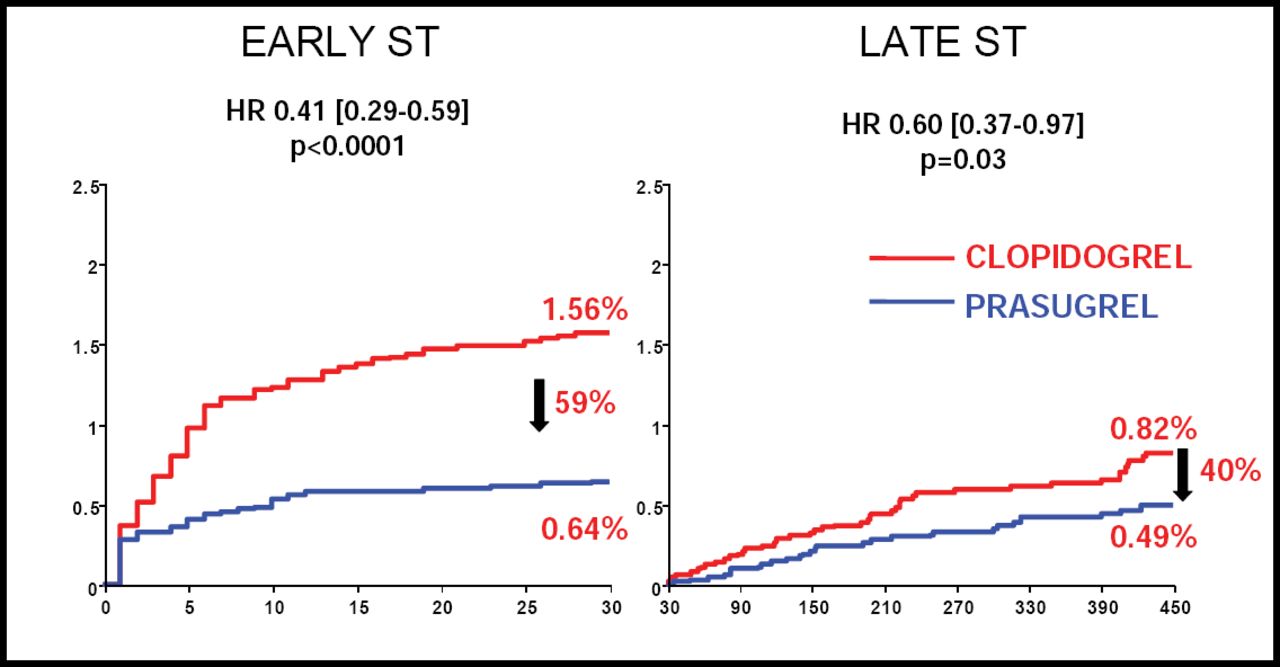
Stephen D. Wiviott, MD, Brigham and Women's Hospital, Boston, MA, reported that the stent analysis portion of TRITON-TIMI 38 demonstrated rates of stent thrombosis for the 2 drugs that were similar to the rates in the main trial. Overall, prasugrel reduced early (within 30 days)stent thrombosis by 59% (0.64% vs 1.56%; p<0.0001) and late stent thrombosis by 40% (0.49% vs 0.82%; p=0.03); (Figure 1). The frequency of definite or probable stent thrombosis associated with prasugrel was significantly lower in the BMS arm (1.27% vs 2.41%; HR 0.52; p=0.0009), as well as in the DES arm (0.84% vs 2.31%; HR 0.36; p<0.0001).

Comparison of Early and Late Definite/Probable Stent Thrombosis (Any stent n=12844).
The rates of stent thrombosis associated with the 2 drugs were also consistent across the various ARC definitions of stent thrombosis. Prasugrel was associated with a 0.9% rate of definite stent thrombosis, a 1.1% rate of definite or probable thrombosis, and a 1.5% rate of definite, probable, or possible thrombosis. All of these rates were significantly lower (p<0.0001) than those for clopidogrel (2.0%, 2.3%, and 2.7%, respectively).
In discussing the balance of efficacy and safety, Dr. Wiviott noted that prasugrel prevented stent thrombosis in 12 of 1000 patients and prevented adverse events other than stent thrombosis (cardiovascular disease, myocardial infarction, and stroke) in 15 of 1000 patients. The drug was associated with major bleeding in 5 of 1000 patients.
“What TRITON-TIMI showed with respect to the prevention of stent thrombosis was clinically very important. Now we need to find ways to determine which patients are best suited for which therapies,” said. Dr. Wiviott.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.