

Summary
The findings of the TAPAS and TRANSFER-AMI Trials have helped to identify ways to improve clinical outcomes of patients with ST-segment elevation myocardial infarction (STEMI) undergoing fibrinolysis or percutaneous coronary intervention (PCI). These studies provide answers about the role of thrombus aspiration before primary PCI and the role and optimal timing of routine PCI after fibrinolysis.
- cardiology clinical trials
- interventional techniques & devices
- myocardial infarction
The findings of 2 studies have helped to identify ways to improve clinical outcomes of patients with ST-segment elevation myocardial infarction (STEMI) undergoing fibrinolysis or percutaneous coronary intervention (PCI). These studies provide answers about the role of thrombus aspiration before primary PCI and the role and optimal timing of routine PCI after fibrinolysis.
Thrombectomy typically is performed before primary PCI in patients with STEMI only when the clot is large. However, the TAPAS trial demonstrated that thrombus aspiration before PCI, regardless of the clot size, resulted in improved myocardial perfusion and better clinical outcomes. TAPAS was a single-center study that involved consecutive patients with STEMI who were randomly assigned to either manual aspiration of the thrombus and PCI (535 patients) or conventional PCI (536 patients). The primary measure of reperfusion was determined by the myocardial blush grade (MBG), and an MBG of 0 or 1 (defined as absent or minimal myocardial blush) was the primary endpoint.
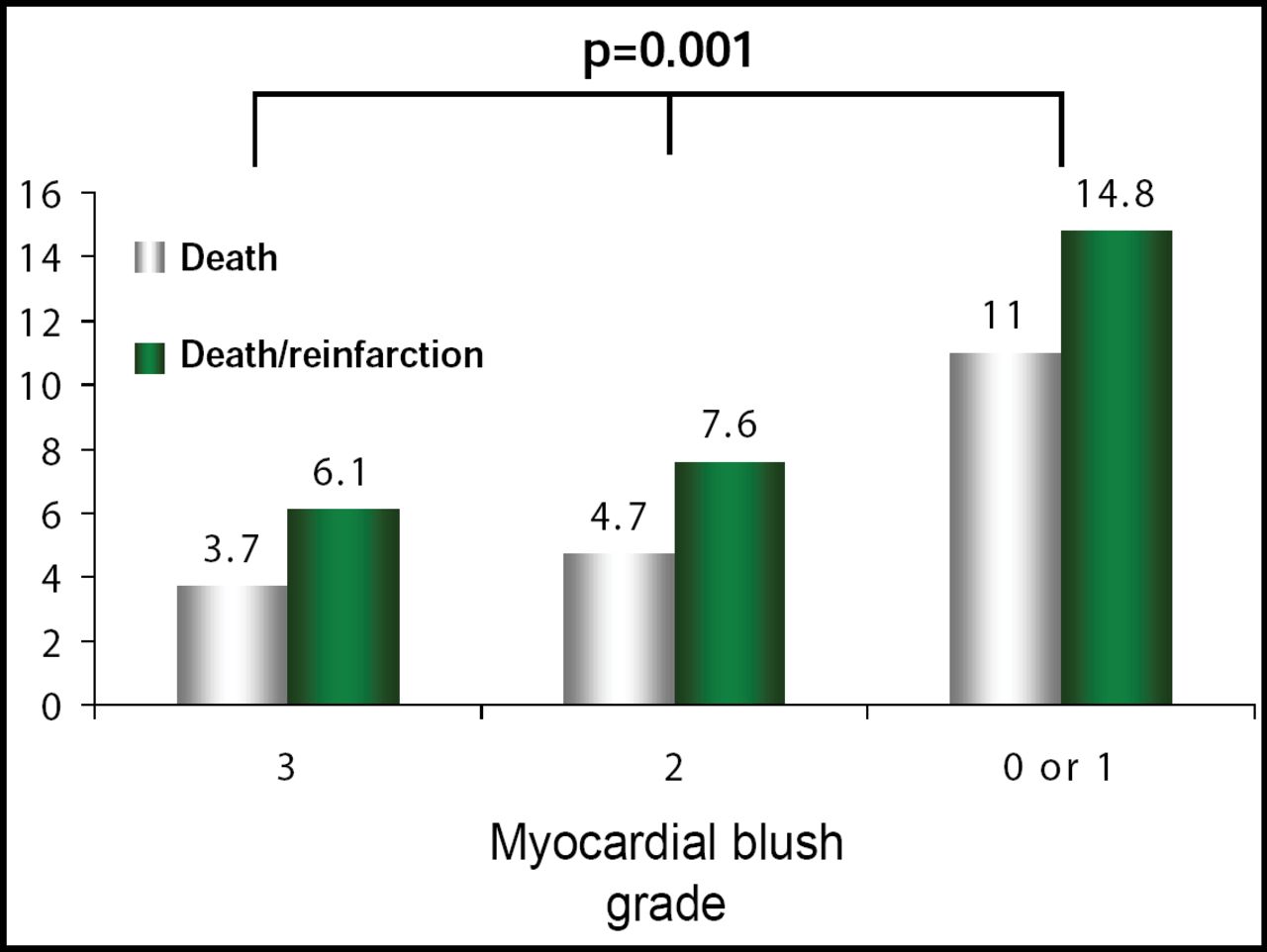
Felix Zijlstra, MD, PhD, Thoraxcentre, University Medical Centre, Groningen, The Netherlands, reported that fewer patients who had thrombus aspiration compared with conventional PCI had an MBG of 0 or 1 (17% vs 26%; p<0.001). Thrombus aspiration also led to a significantly higher rate of complete resolution of ST-segment elevation, another measure of myocardial reperfusion (57% vs 44%; p<0.001). Through 30 days, thrombus aspiration tended to reduce the risk of death (RR 0.52; p=0.07), reinfarction (RR 0.40; p=0.11), target-vessel revascularization (RR 0.77; p=0.34), and major adverse cardiac events (RR 0.72; p=0.12). At one year, the rate of the composite endpoint (death and reinfarction) was significantly lower among patients who had thrombus aspiration (Figure 1). In addition, MBG was found to be a good predictor of clinical outcome; the one-year mortality rate was significantly lower for patients with an MBG of 3 than for patients with a MBG of 0/1 (3.7% vs 11%; p=0.001).

TAPAS One Year Outcome: Myocardial Blush Grade and Death or Death/Reinfarction at 1 Year.
The TRANSFER-AMI trial was designed to determine the optimal timing of PCI after fibrinolytic therapy for patients with STEMI. The study involved patients who initially presented to centers that did not have timely access to a catheterization laboratory. The patients were randomly assigned to one of 2 treatment strategies. The first group (522 patients) received a pharmacoinvasive approach that consisted of fibrinolytic therapy (standard-dose tenecteplase and aspirin [160–325 mg]) and transfer for PCI within 6 hours. The control group (508 patients) received the same fibrinolytic therapy, with rescue PCI performed only if necessary (ongoing chest pain and <50% resolution of ST-elevation at 60–90 minutes, or if the patient was hemodynamically unstable).
Warren J. Cantor, MD, St. Michael's Hospital, Toronto, Ontario, Canada, reported that the incidence of the primary endpoint (a composite of 30-day death, MI, heart failure, severe recurrent ischemia, or shock) in the pharmacoinvasive arm was about half of the rate observed with standard treatment (HR: 0.54, 95% CI, 0.37–0.73; p=0.0013). Evaluation of the individual elements of the endpoint showed that the rates of death, shock, and new or worsening heart failure were not significantly different in the two arms, while the rates of reinfarction and recurrent ischemia were lower in the pharmacoinvasive arm (Table 1). Thrombolysis in Myocardial Infarction (TIMI) major bleeding occurred at similar rates in the 2 arms (4.3% vs 4.6%; p=0.88). These findings support the strategy of transfer to a PCI center immediately after fibrinolysis, without waiting to see whether reperfusion is successful, said Dr. Cantor.
Comparison of the Results for the 2 Treatment Arms in the TRANSFER-AMI Trial.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.