

Summary
Intensified NT-BNP (N-terminal B-type natriuretic peptide)-guided therapy is not more effective than standard, symptom-guided therapy in reducing death and all-cause hospitalization among elderly congestive heart failure patients, according to results from the Trial of Intensified [BNP-guided] versus standard [symptom-guided] Medical therapy in Elderly patients with Congestive Heart Failure [TIME-CHF; ISRCTN43596477].
- cardiology clinical trials
- heart failure
Intensified NT-BNP (N-terminal B-type natriuretic peptide)-guided therapy is not more effective than standard, symptom-guided therapy in reducing death and all-cause hospitalization among elderly congestive heart failure (CHF) patients, researchers reported at the European Society of Cardiology (ESC) Congress 2008 in Munich. However, response to treatment differed between age groups, wherein patients aged 60 to 74 years achieved significantly reduced mortality and improved survival free of hospitalization for heart failure (HF) in contrast to with subjects aged 75 years and older, where there was no difference between the two treatment strategies.
“Intensified BNP-guided therapy may be considered in younger patients to reduce disease-specific risk and mortality,” said presenter and trial leader Hans-Peter Brunner-La Rocca, MD, University Hospital, Basel, Switzerland. “However, patients over 75 show no benefit,” he added.
Dr. Brunner-La Rocca noted that previous studies had suggested a possible outcome benefit for HF patients who were treated with BNP-guided therapy. The purpose of this study was to test this hypothesis specifically in an elderly population.
Such research is particularly important in elderly patients, who are physically less active and in whom symptoms are more obscure. Dr. Brunner-La Rocca also emphasized that even though elderly patients represent the majority of HF patients, they have been underrepresented in randomized trials thus far.
Investigators for TIME-CHF (Trial of Intensified [BNP-guided] versus standard [symptom-guided] Medical therapy in Elderly patients with Congestive Heart Failure; ISRCTN43596477) enrolled 499 Swiss and German subjects from 15 participating hospitals in the 18-month study. Enrollment criteria included patients aged 60 or older (with no upper limit), symptomatic HF, New York Heart Association (NYHA) ≥ class II despite therapy, left ventricular ejection fraction (LVEF) ≤45%, HF hospitalization within the last year, and elevated NT-BNP (>400 pg/ml for those aged 60 to 74 years and >800 pg/ml for those aged 75 years and older).
Exclusion criteria included dyspnea that was not mainly caused by CHF, significant uncorrected valvular heart disease, acute coronary syndrome within 10 days, angina pectoris due to ischemia, PCI (percutaneous coronary intervention) within 1 month or CABG (coronary artery bypass graft surgery) within 3 months, body mass index >35, serum creatinine >2.5 mg/dl and life expectancy of less than 3 years (unrelated to cardiovascular disease).
Participants were randomized to standard versus intensified therapy and stratified by age (75 years and older vs 60 to 74 years). Primary study endpoints were survival free of any hospitalization and quality of life with secondary endpoints of survival and survival free of HF hospitalization.
The aim of therapy in the standard treatment group (n=248) was NYHA ≤II, blinded to NT-BNP results. The aim in the intensified treatment group (n=251) was NT-BNP <400 pg/ml (60–74 years) or <800 pg/ml (75 years and older) and NYHA ≤II.
The mean age of all subjects was 76 years, and 35% were female. At baseline, 55% of all subjects had been diagnosed with kidney disease and 77% had 2 or more clinically relevant comorbidities.
Subjects were treated according to ESC Guidelines with ACE [angiotensin-converting enzyme] inhibitors (ARB [angiotensin receptor blocker], if ACE inhibitors not tolerated), beta-blockers, and spironolactone (for persistent NYHA >III, eplerenone if not tolerated) in adequate doses.
In both the standard and intensified treatment groups at baseline, 95% of the subjects were on ACE inhibitor/ARB therapy, with 81% and 76%, respectively, also on beta-blocker therapy. In both stratified age groups, 95% of subjects were on ACE inhibitor/ARB therapy, with 84% in the younger group and 75% in the older group on beta-blocker therapy.
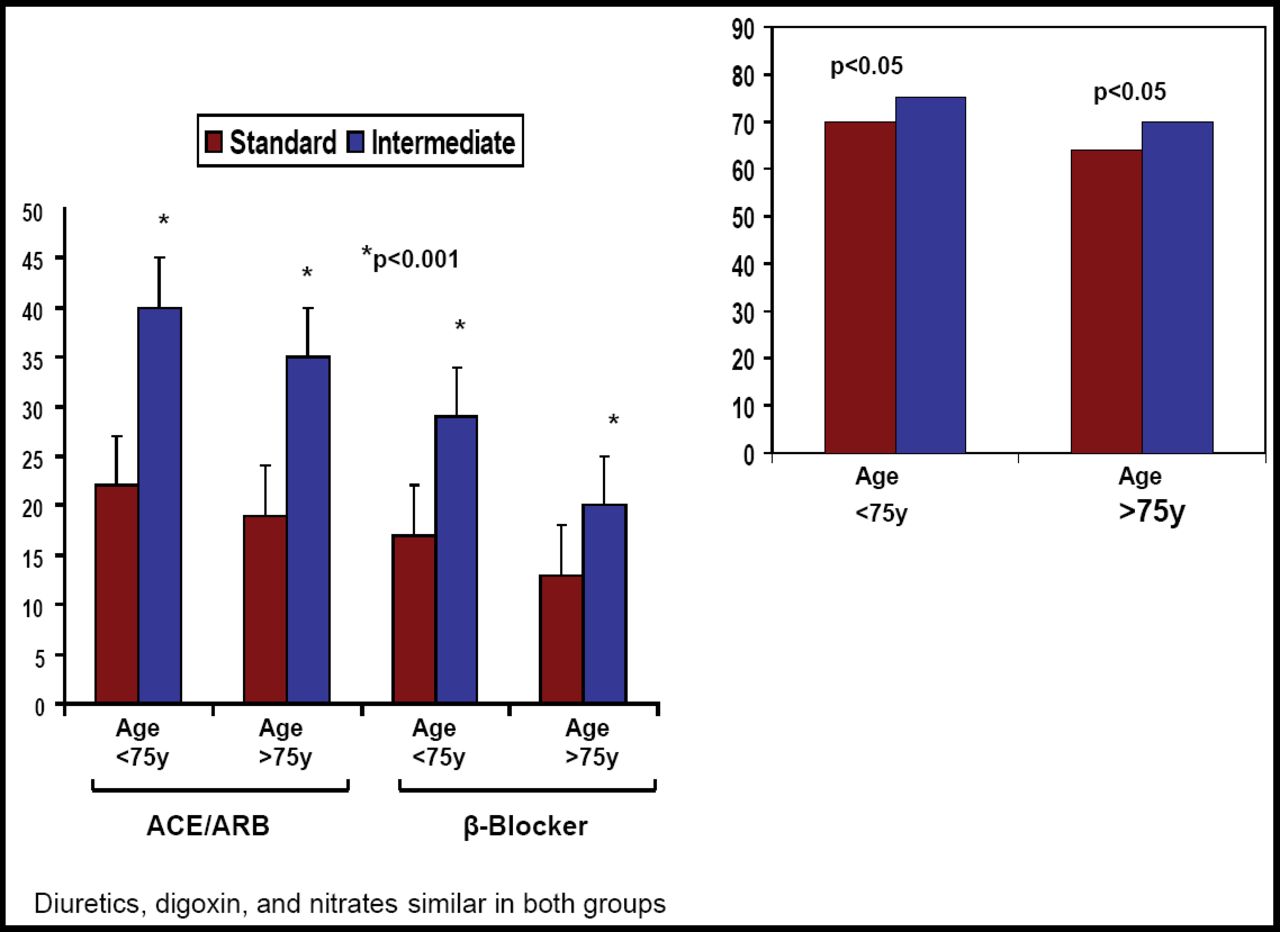
Dr. Brunner-La Rocca reported a significant increase in ACE inhibitor/ARB and beta-blocker doses among BNP-guided therapy subjects compared with standard treatment subjects (p<0.001), as well as a comparative increase in mineral corticosteroid antagonist (MCA) use (p<0.05) between the 2 groups. Diuretic, digoxin, and nitrate use was similar in both groups.
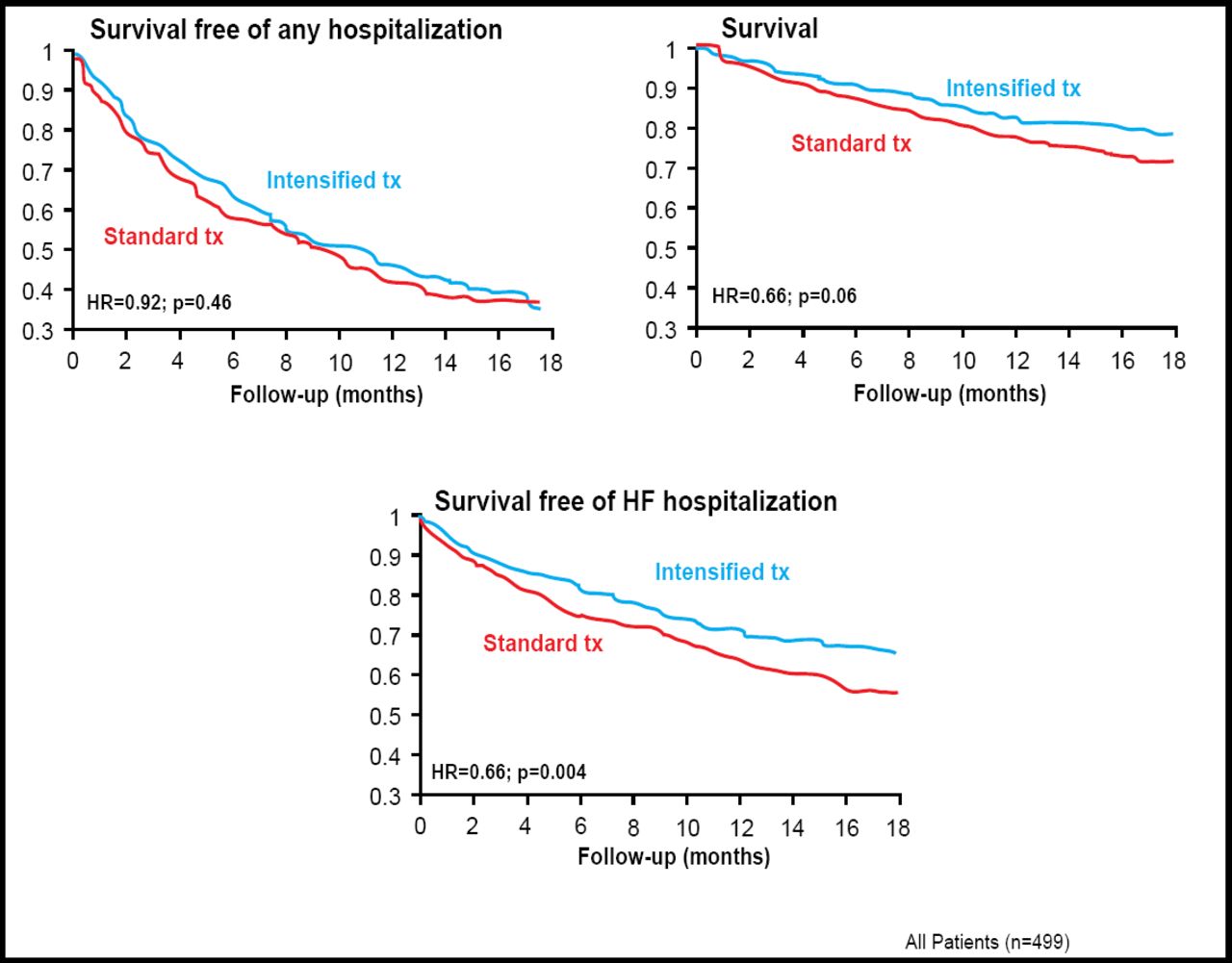
Dr. Brunner-La Rocca reported that there was no improvement by intensified BNP-guided therapy on the primary endpoint of survival free of hospitalization (HR=0.92; p= 0.46). However, he reported an improvement with intensified BNP-guided therapy on the secondary endpoints of survival (HR=0.68; p=0.06) and survival free of HF hospitalization (HR=0.66; p=0.008; Figure 1).
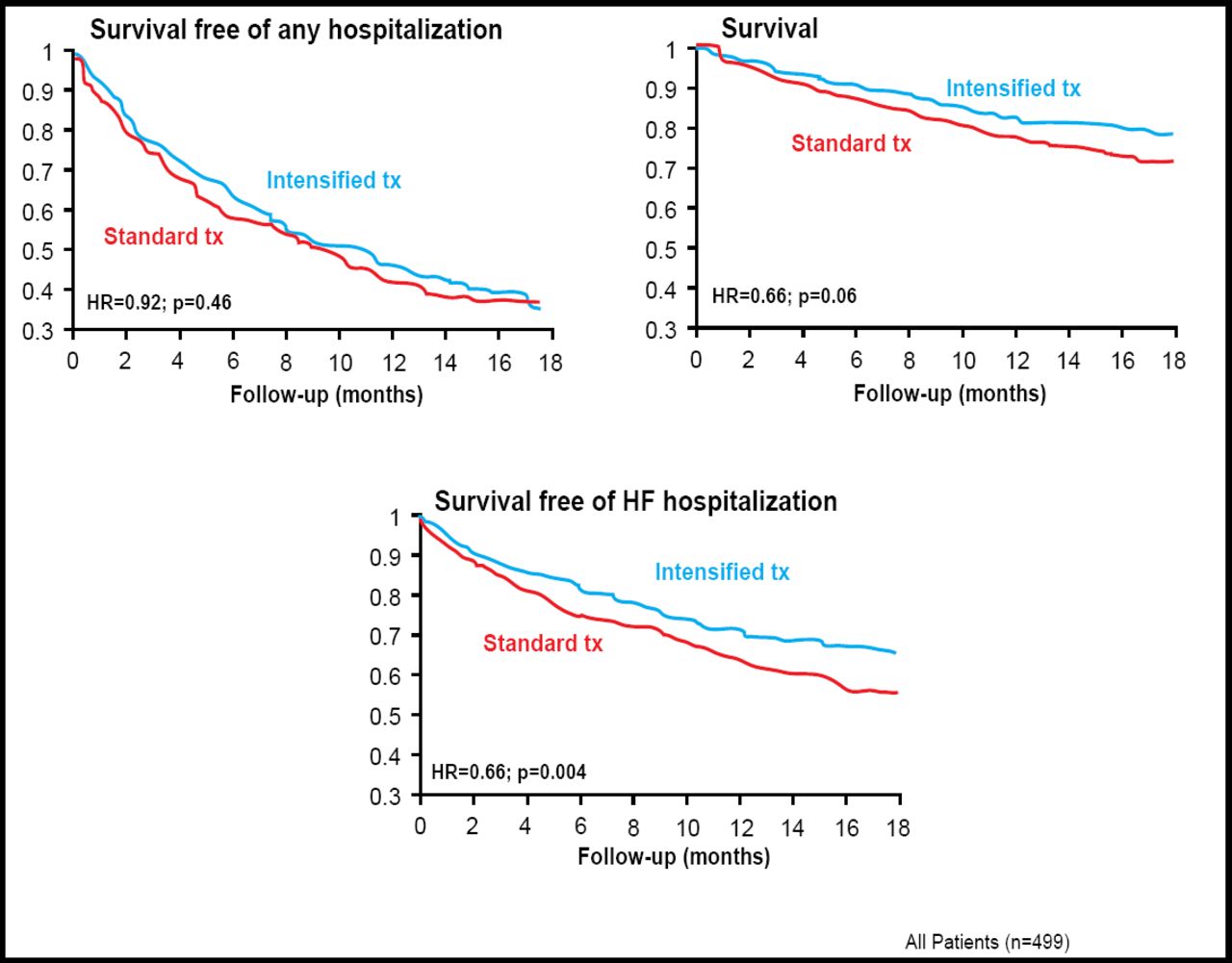
Study Endpoints. All Patients.
He also reported that when the results were stratified by age (60 to 74 years vs 75 and older), there was a significant difference between the 2 age groups. Whereas there was significant improvement in survival (HR=0.38 [95% CI, 0.18 to 0.80]; p=0.01) and in survival free of HF hospitalization (HR=0.41; 95% CI, 0.23 to 0.72; p=0.002) in younger patients no effect of the treatment strategies was seen in elderly subjects (Figure 2).
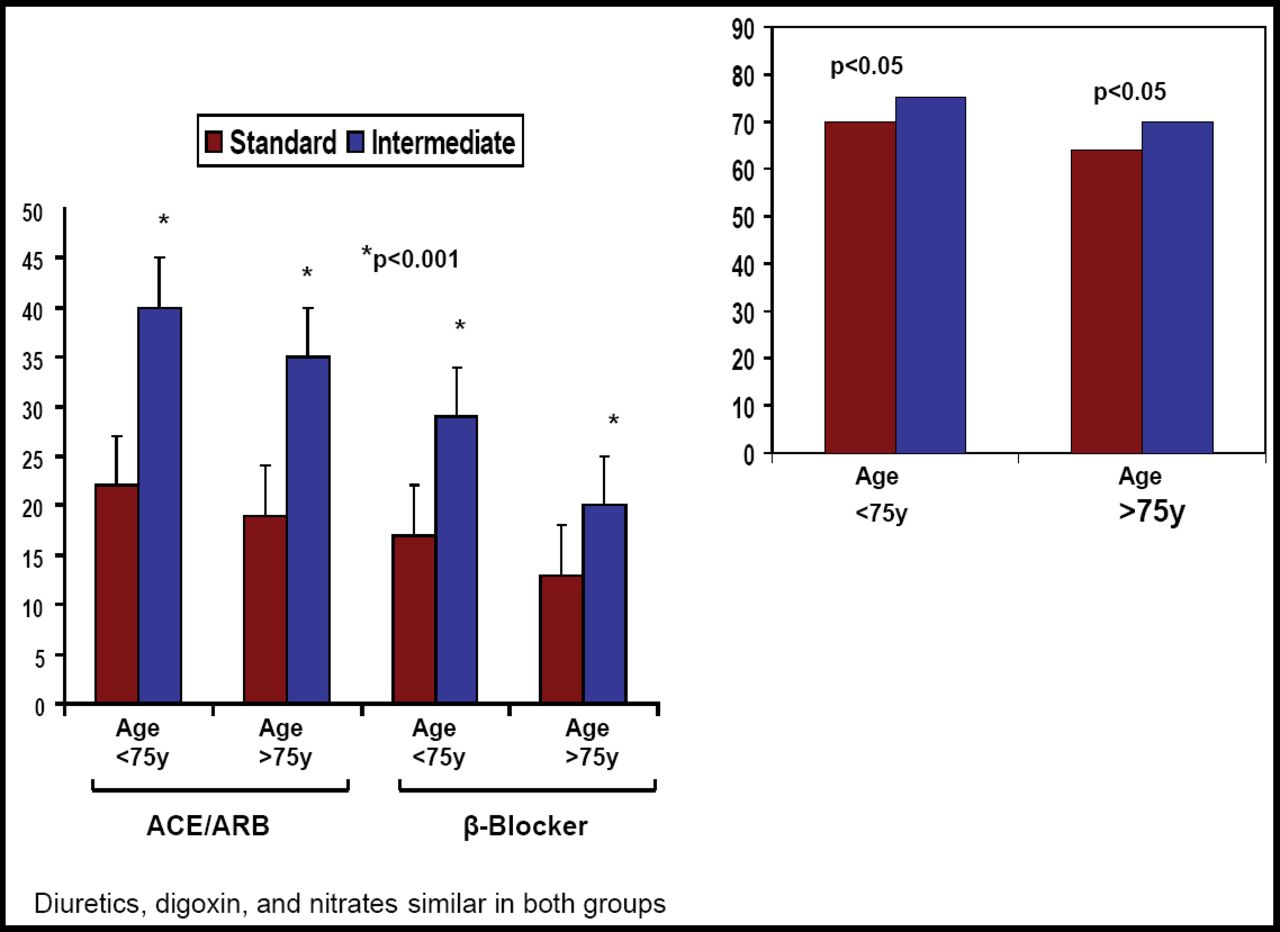
Dosage Increase Stratified According To Age.
The quality-of-life primary endpoint showed improvement in all patients regardless of treatment. However, improvement in quality of life was significantly lower in the older (≥75 years) intensively treated patients compared with older patients on symptom guided therapy (interaction p<0.05).
Dr. Brunner-La Rocca concluded that this study shows that evidence from HF trials in younger patients “may not simply be applied to older patients. We need specific heart failure trials in elderly patients, and I hope that this study will stimulate further trials in this regard.”
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.