

Summary
Obstructive sleep apnea, which is prevalent among patients with type 2 diabetes, has been found to be significantly associated with peripheral neuropathy and retinopathy—two diabetes-related complications that cause substantial morbidity. The findings are from two studies that were conducted in the diabetes clinic of a UK-based hospital.
- Sleep Disorders
- Diabetes Mellitus
Obstructive sleep apnea (OSA), which is prevalent among patients with type 2 diabetes, has been found to be significantly associated with peripheral neuropathy and retinopathy—two diabetes-related complications that cause substantial morbidity. The findings are from two studies that were conducted in the diabetes clinic of a UK-based hospital, and Abd Tahrani, MD, MRCP, MMedSci, University of Birmingham, United Kingdom, reported the results.
OSA occurs in as many 86% of people with type 2 diabetes. Because OSA and diabetes complications share common inflammatory and molecular consequences, Dr. Tahrani and coinvestigators hypothesized that OSA may aggravate microvascular dysfunction and cellular damage in diabetes, resulting in peripheral neuropathy and retinopathy.
OSA in Patients with Type 2 Diabetes: A Novel Predictor of Peripheral Neuropathy
Data from 231 patients with diabetes were analyzed. Patients with known respiratory disorders (including OSA) were excluded, as were patients who were known to have neuropathy for reasons other than diabetes. Diabetic peripheral neuropathy (DPN) was diagnosed using the Michigan Neuropathy Screening Instrument, and OSA was assessed using home-based portable multichannel respiratory monitoring [ADA 2011. Poster 0388-PP].
The overall prevalence of OSA was 64.5%. Of the 149 patients with OSA, 59% had mild apnea, as measured by the apnea-hypopnea index (AHI 5 to <15 events); 23% had moderate apnea (AHI 15 to <30 events), and 18% had severe apnea (AHI ≥30 events).
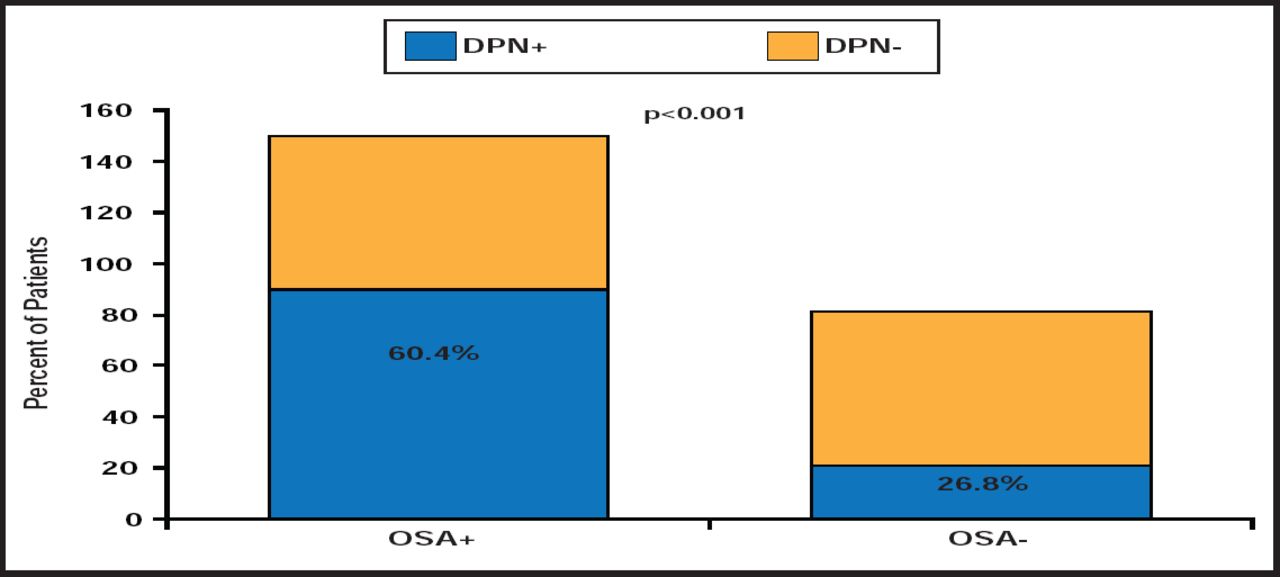
The overall prevalence of DPN was 45%. The prevalence was significantly higher among patients with OSA than those without OSA (p<0.001; Figure 1). Patients with OSA reported more neuropathic symptoms, and all aspects of the foot exam and the prevalence of skin hypersensitivity were more common among patients with OSA. The severity of peripheral neuropathy was found to correlate with the severity of OSA.

The Relationship Between OSA and DPN.
Reproduced with permission from A. Tahrani, MD, MRCP, MMedSci.
The unadjusted odds ratio (OR) for peripheral neuropathy was 4.160 (95% CI, 2.309 to 7.494; p<0.001). After adjustment for possible confounders (including age, gender, waist circumference, smoking and alcohol, diabetes duration, medications, and other factors), OSA remained an independent predictor of peripheral neuropathy (OR=2.958; 95% CI, 1.416 to 6.178; p=0.004).
OSA in Patients with Type 2 Diabetes: A Novel Predictor of Sight Threatening Retinopathy
The results of a study on retinopathy were similar [ADA 2011. Poster 0391-PP]. Among 224 patients in the study, the overall prevalence of OSA was 63%. Of the 142 patients with OSA, 61.3% had mild apnea, 23.2% had moderate apnea, and 15.5% had severe apnea.
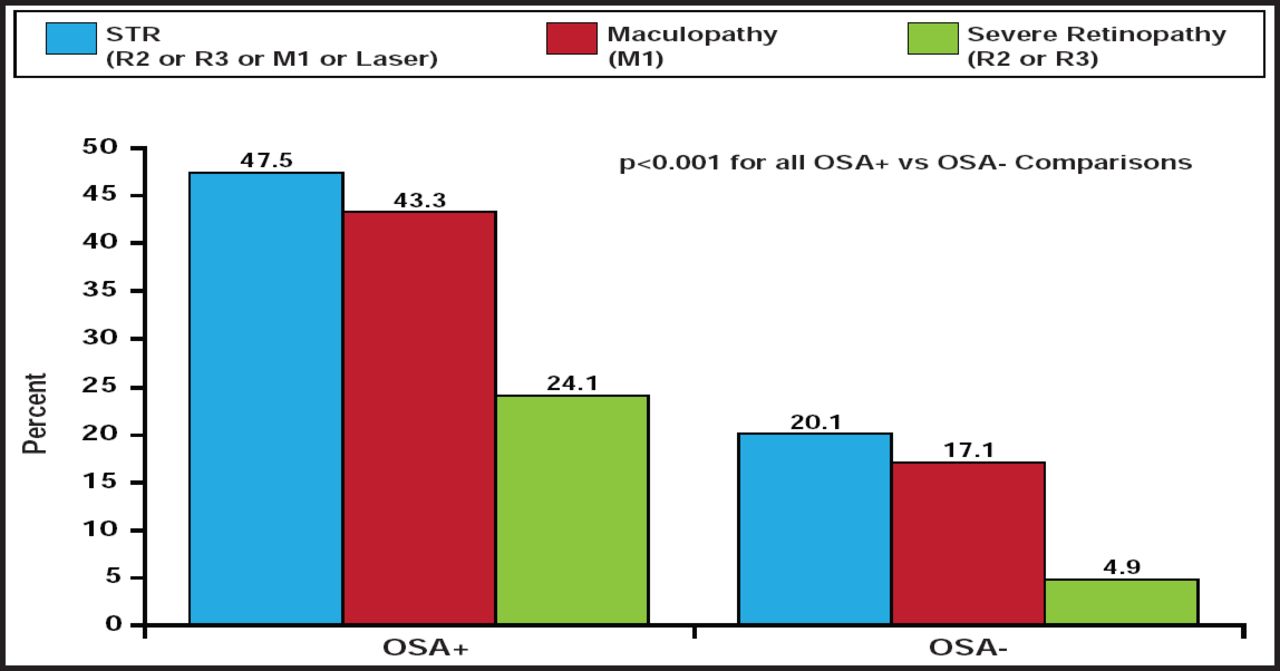
Rates of sight-threatening retinopathy, severe retinopathy, and maculopathy were determined on the basis of screening images or an ophthalmologist diagnosis. The overall prevalence of each oculopathy was 37.4%, 16.2%, and 33.7%, respectively. The prevalence of each oculopathy was significantly higher among patients with OSA than among those without OSA (Figure 2).

The Relationship Between OSA and Sight-Threatening Retinopathy, Diabetic Retinopathy, and Maculopathy.
Reproduced with permission from A. Tahrani, MD, MRCP, MMedSci.
After adjustment for possible confounders, OSA was an independent predictor of each oculopathy:
-
Sight-threatening retinopathy: OR=3.633 (95% CI, 1.642 to 8.037; p=0.001)
-
Severe retinopathy: OR=5.057 (95% CI, 1.380 to 18.537; p=0.014)
-
Maculopathy: OR=4.443 (95% CI, 1.925 to 10.253; p<0.001)
The data from the two studies suggest that OSA may play an important role in the development of both diabetic neuropathy and retinopathy. Prospective studies are needed to confirm this hypothesis. In addition, research is needed to determine the impact of treating OSA on both diabetic complications.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.