

Summary
Approximately 0.4–2% of the European population has heart failure (HF), representing more than 14 million people. Another 4–5 million people in the United States are affected. The prognosis for older patients with HF is similar to that for severe malignant diseases, with a median survival of less than 5 years [Thomas et al. Heart Fail Clin 2007]. This article discusses definitions and classification, pharmacologic therapies, prognostic factors, and patient education.
- heart failure

“Heart failure is probably the most important cause of death and disability, and the most important [factor] in health economics,” says Kim Fox, MD, Royal Brompton Hospital, London, UK, and 2006–2007 President of the European Society of Cardiology (ESC). Approximately 0.4–2% of the European population has heart failure (HF), representing more than 14 million people. Another 4–5 million people in the United States are affected. The prognosis for older patients with HF is similar to that for severe malignant diseases, with a median survival of less than 5 years [Thomas et al. Heart Fail Clin 2007].
“Heart failure is our most clinically relevant problem,” adds Jeroen Bax, MD, Leiden University Medical Center, the Netherlands, and Chair of the ESC Congress Program Committee. The multifaceted nature of HF adds to the challenge in diagnosis, according to Ken Dickstein, MD, President of the Heart Failure Association of the ESC. “The complexity of Heart failure is a major obstacle to adequate identification and diagnosis of untreated patients,” he said, explaining that HF is not a disease but a syndrome of many converging etiologies. Ischemic heart disease is the cause of HF in approximately 60–70% of patients, especially older patients; dilated cardiomyopathy is a common cause among younger patients.
Definition and Classification
“There is no globally accepted definition and classification of acute Heart failure,” says Markku Nieminen, MD, University Central Hospital, Helsinki, Finland. Several HF classifications have been established, but each is based on specific sets of clinical features and applies to selected patient populations, he adds. For example, the Killip classification, based on clinical signs and chest x-ray findings, and the Forrester classification, based on clinical signs and hemodynamic characteristics, are best applied to acute de novo HF [Killip T 3rd et al. Am J Cardiol 1967; Forrester JS et al. Am J Cardiol 1977]. In contrast, the “US classification,” based on clinical findings, is most applicable to acutely decompensated chronic HF [Nohria A et al. JAMA 2002].
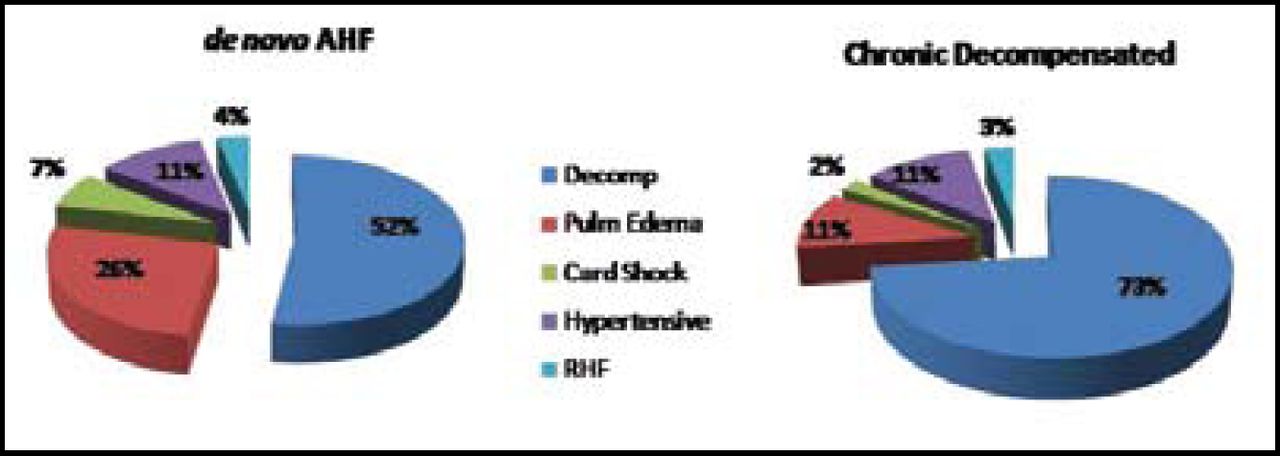
Both de novo and chronic HF are associated with several distinct clinical conditions, including hypertension, pulmonary edema, cardiogenic shock, high output failure, and right HF. According to the EuroHeart Failure Survey II, the prevalence of these conditions differs between the two types of HF (Figure 1) [Nieminen MS et al. Eur Heart J 2006].

Distribution by Presentation.
In addition, acutely decompensated chronic HF is associated with a significantly higher prevalence of background diseases, especially coronary artery disease, atrial fibrillation, valvular disorder, renal failure, anemia, chronic obstructive pulmonary disease, and the presence of a pacemaker. As a result, Prof. Nieminen points out, cases of acutely decompensated chronic HF are complicated, whereas cases of de novo HF are more severe, but acute.
The 2005 ESC guidelines clearly delineate the clinical groups and severity manifestations within HF, notes Prof. Nieminen, and therapy and prognosis differ for these clinical groups [Nieminen MS et al. Eur Heart J 2005].
Pharmacologic Therapy
“We need to optimize treatment for patients with acute decompensated chronic heart failure” says John T. Parissis, MD, Attikon University Hospital, Athens, Greece. The goal of treatment, he says, is to improve symptoms without promoting mechanisms of myocardial injury and cardiac remodeling. Vasodilators remain the gold standard. Other classes of drugs commonly used in the initial management of HF include diuretics (furosemide, bumetanide, or torasemide) and inotropic agents (beta-agonists [dobutamine, dopamine] and phosphodiesterase inhibitors [milrinone]). Many of these drugs are useful for the treatment of acute symptoms and have improved short-term hemodynamic characteristics, but several studies have indicated that some are associated with decreases in survival and/or increases in cardiovascular and renal events.
Vasodilators
Nesiritide is the newest class of vasodilator developed for the treatment of HF. However, Prof. Parissis notes that a meta-analysis has shown that it is associated with significant worsening of renal function and a significantly higher mortality rate [Sackner-Bernstein JD et al. JAMA 2005].
Inotropic Agents
Current intravenous inotropic therapies improve clinical symptoms and hemodynamics but have been associated with increased long-term mortality, says Prof. Parissis. Other adverse events include myocardial injury, adverse interaction with beta-blockers, and arrhythmogenesis.
One new inotropic drug, levosimendan, seems to be more effective than traditional inotropes in improving cardiac mechanical efficiency and reducing congestion without causing cardiomyocyte death or increasing myocardial oxygen uptake. Levosimendan has been evaluated in several large-scale studies, such as LIDO, REVIVE I and II, and SURVIVE. In all of these studies, levosimendan has been associated with improved clinical outcome and hemodynamics; in addition, survival was improved in LIDO [Follath F et al. Lancet 2002; DeLuca L et al. Eur Heart J 2006; Mebazaa A et al. JAMA 2007]. In his own study, Prof. Parissis found that levosimendan prevents oxidative damage, which may contribute to HF deterioration [Parissis JT et al. Atherosclerosis 2007].
Investigational Agents
Several investigational drugs targeted to novel pathophysiologic mechanisms have shown promise in early trials, says Prof. Parissis (Table 1). The findings of ongoing trials will help define their clinical efficacy and safety.
Investigational Agents Targeting Novel Pathophysiologic Mechanisms in Heart Failure.
Statins
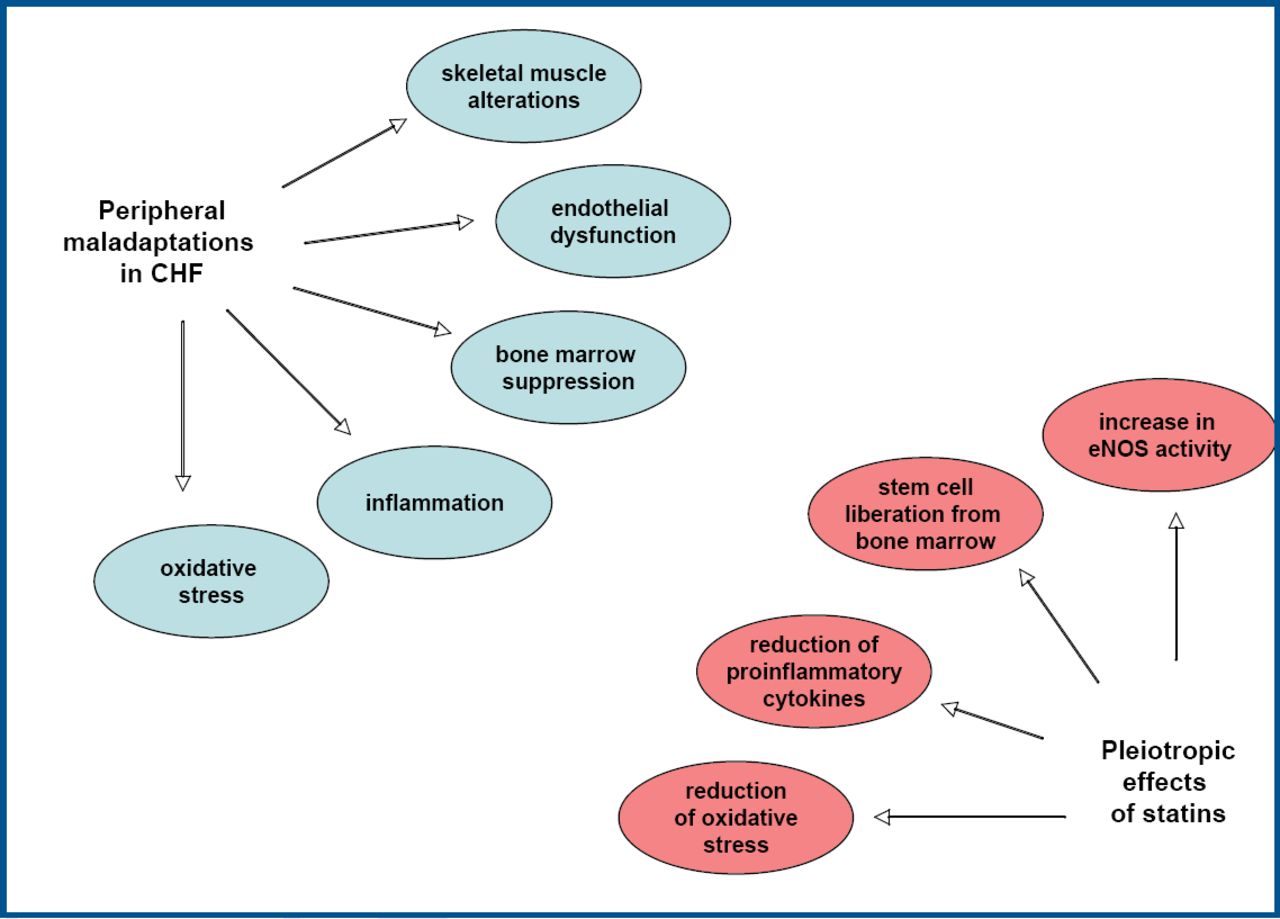
Statins have been shown to have benefit for HF patients beyond their role in preventing additional acute coronary events [Scirica et al. J Am Coll Cardiol 2006; Khush et al. Circulation 2007]. Research indicates that the pleiotropic effects of statins lead to improvement in many of the peripheral maladaptations of chronic HF, says Sandra Erbs, MD, University of Leipzig, Germany (Figure 2).

Pleiotropic Effects of Statins in Peripheral Maladaptations of CHF.
In a study of patients with chronic HF, Prof. Erbs and colleagues found that rosuvastatin decreased oxidative stress in the blood and increased the number and function of circulating stem and progenitor cells. “The rosuvastatin-mediated correction…was linked to a partial reversal of left ventricular remodeling and an improvement in central hemodynamics,” noted Prof. Erbs.
Statins have also been shown to be associated with significantly lower all-cause mortality, according to a study conducted by Professor S. Maini, Taunton Hospital, UK, and colleagues. The effect was irrespective of age, sex, thrombolysis, other drugs, revascularization, or presence of an implantable device. In addition, research led by Ralph Winkler, MD, Medizinische Klinik B, Germany, has shown that statins improve outcomes in both preserved and impaired left ventricular function settings. In evaluating 18,936 patients with ACS-related HF, Prof. Winkler and colleagues found that treatment with statins reduced mortality at 14 months by 50%. “The lower the left ventricular ejection fraction, the higher the benefit of statin treatment,” says Prof. Winkler, noting that the number needed to treat for an ejection fraction <30% was 8 vs 42 for an ejection fraction >55%.
Although current European guidelines for the management of chronic HF do not include recommendations regarding the use of statins, Prof. Winkler notes that they should be prescribed according to guidelines for the treatment of ACS.
Agents to Improve Functional Capacity
Despite advances in treatment, patients with chronic HF have a poor quality of life and low exercise tolerance. To address these issues, investigators have been evaluating the potential of pharmacologic agents to improve functional capacity. Nadine Clausell, MD, Hospital de Clinicas de Porto Alegre, Brazil, reports that treatment with sildenafil for 4 weeks improved the functional capacity and decreased secondary pulmonary hypertension in patients with New York Heart Association (NYHA) class I-III HF and left ventricular ejection fraction ≤40%. After 4 weeks of treatment with sildenafil (50 mg TID), VO2 increased 13% and pulmonary artery systolic pressure decreased 32%.
Functional capacity was also improved in men older than 60 years with NYHA class I-III HF who received testosterone (one intramuscular injection of undecanoate). Giuseppe Caminiti, MD, IRCCS, San Raffaele, Italy, reports that at 3 months, distance on the 6-minute walk test improved vs baseline for men who had received testosterone and optimal medical therapy (from 387 meters to 499 meters) vs men who received placebo and optimal medical therapy (from 391 meters to 428 meters). Muscle strength and glucose metabolism were also improved. The benefits of testosterone seem to be mediated by metabolic and peripheral effects, says Prof. Caminiti. An important next step would be to test promising therapies such as sildenafil and testosterone in randomized controlled trials designed to assess their effect on clinical outcomes such as rehospitalization for HF and death.
Prognostic Factors
Prognostic models have demonstrated a wide variety of patient-related and disease-related factors that predict mortality in HF. A better understanding of these factors may improve outcomes through enhanced treatment plans.
“Therapy especially targeted at preservation and improvement of renal function may…provide a new possibility to improve prognosis in patients with HF,” says K. Damman, MD, University Medical Center Groningen, the Netherlands. Prof. Damman and colleagues conducted a meta-analysis and found that worsening renal function was associated with an increase in all-cause mortality and hospitalization. Furthermore, the risk of mortality rose with increasing severity of worsening renal function, and patients with impaired renal function at baseline were at increased risk for worsening renal function.
The importance of monitoring weight in patients with HF was reinforced by the findings of a study in which weight loss and leanness simultaneously predicted poor prognosis in a broad spectrum of HF patients. The study was carried out by Joanna Dobson, MD, London School of Hygiene, UK, who reports that weight loss at 6 months predicted poor prognosis in the long-term. In the study, for every 1% weight loss, there was an 11.2% increase in mortality hazard. Prof. Dobson advocates for more intense monitoring of weight loss as well as optimizing treatment when weight loss is detected.
Patient Education
According to the Study group on Heart failure Awareness and Perception in Europe (SHAPE) study, only 3% of 7,958 respondents to a European survey could correctly identify HF from a description of typical signs and symptoms [Remme WJ et al. Eur Heart J 2005]. This was much lower than the rates for recognition of any other cardiovascular disease. To address this knowledge gap, the Heart Failure Association of the ESC developed the website www.heartfailurematters.org. “The website is designed to empower patients to know what they can do to help themselves,” says Prof. Dickstein. It offers a description of HF and its treatment in simple language and features an optional narrative guide to help older visitors to the site. Prof. Dickstein encouraged physicians to tell their patients about the website as a way to improve patient compliance with treatment and lifestyle changes that can help enhance their quality of life and improve survival.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.