

Summary
This article discusses the renewed focus on treatment-resistant hypertension (RH), which has been sparked by the interest in catheter renal denervation and the somewhat disappointing results with this interventional approach in the SYMPLICITY HTN trial program.
- Renal Disease
- Interventional Techniques & Devices
- Hypertension & Kidney Disease
- Hypertensive Disease
- Renal Disease
- Interventional Techniques & Devices
- Hypertension & Kidney Disease
- Hypertensive Disease
- Cardiology
Four leading hypertension experts voiced their hope for a renewed focus on treatment-resistant hypertension (RH), sparked by the interest in catheter renal denervation (RDN) and the somewhat disappointing results with this interventional approach in the SYMPLICITY HTN trial program.
The prognosis of RH is severe, stated Roland E. Schmieder, MD, Friedrich Alexander University, Erlangen, Nurnberg, Germany, with associated annual rates of all-cause death ranging from 2% to 4% and major adverse cardiovascular (CV) and cerebrovascular events of 4.6%, on the basis of estimates from retrospective analyses, as there are no prospective, observational, longitudinal data.
RH is defined by the major hypertension guidelines as a blood pressure (BP) that remains above goal despite optimized treatment with ≥3 antihypertensive (AH) drugs from different drug classes, including a diuretic. The European Society of Hypertension (ESH) and European Society of Cardiology (ESC) Guidelines include appropriate lifestyle measures in their definition [Mancia G et al. J Hypertens 2013].
In the international Reduction of Atherothrombosis for Continued Health registry, patients identified as having RH (12.7% of 53,530 patients) had an increased risk for CV death, myocardial infarction, or stroke at 4 years compared with patients without RH (HR, 1.11; 95% CI, 1.02 to 1.20; p=0.017) [Kumbhani DJ et al. Eur Heart J 2013]. An increased risk was noted for the individual endpoints of nonfatal stroke (HR, 1.26; 95% CI, 1.10 to 1.45; p= 0.0008) and hospitalization for congestive heart failure (p<0.0001).
Adherence to treatment is a key factor to distinguish between uncontrolled hypertension (UH) and true RH. UH is defined as a lack of BP control despite treatment because of inadequate treatment regimens, poor adherence, undetected secondary hypertension, and true RH. One study showed that 23% of patients with RH were only partially adherent and 24% were fully nonadherent to treatment [Strauch B et al. J Hypertens 2013]. Other studies have investigated whether tandem high-performance liquid chromatography/mass spectrometry urine analysis could be used to assess medication adherence and differentiate between patients with true RH versus UH due to nonadherence [Tomaszewski M et al. Heart 2014].
An analysis from a community-based practice network in the United States showed that only 15% of 468,877 patients with hypertension had been prescribed optimal treatment; 31.5% had UH despite ≥3 AH drugs [Egan BM et al. Hypertension 2013].
In the United States, the prevalence of apparent RH rose from 15.9% in the period from 1998 to 2004 to 28.0% in the period from 2005 to 2008 among 13,375 adults treated with ≥3 drugs in the National Health and Nutrition Examination Surveys [Egan BM et al. Circulation 2011]. Clinical characteristics associated with RH were albuminuria, reduced renal function, and signs of target organ damage. Prof. Schmieder stated that this increase in RH reflects improved efforts to treat patients to target BP levels, rather than a sicker population.
In the Spanish Ambulatory Blood Pressure Monitoring Registry of 68,045 treated patients with UH in usual daily practice, 12.2% had RH on the basis of office BP (OBP) ≥140/90 mm Hg despite predefined background therapy, while it was lower (7.6%) on the basis of ambulatory BP monitoring (ABPM) [de la Sierra A et al. Hypertension 2011]. The investigators suggested that ABPM may be a way to distinguish between true RH and white-coat hypertension.
The discordance between OBP and ABPM in distinguishing patients with RH was also found in the 3A Registry and thus requires further investigation, said Prof. Schmieder. Among 14,988 patients with UH enrolled in the registry, 1628 were taking ≥3 AH drugs at 1-year follow-up. Of these, BP was controlled in 49.63% on the basis of OBP and ABPM. However, in 5.65%, BP was controlled on the basis of OBP but not ABPM. Furthermore, 29.3% had UH on the basis of OBP but not ABPM, and 15.42% had controlled hypertension on the basis of ABPM but not OBP.
Screening for secondary forms of hypertension is essential because they are frequent in the setting of RH, stated Michel Azizi, MD, Paris Descartes University, Hôpital Européen Georges Pompidou, Paris, France. Primary aldosteronism is the most frequent cause of RH (20%–30%) and may be curable in younger patients with aldosterone-producing adenomas. The screening test is based on the measurement of the plasma aldosterone-to-renin ratio. The diagnosis of aldosterone-producing adenoma is based on additional tests to confirm autonomous aldosterone secretion (saline infusion test) and on imaging procedure (computed tomographic or magnetic resonance angiography [CTA; MRA]), followed by confirmation of the lateralization of aldosterone secretion by adrenal vein sampling in case of indication of adrenal surgery. Other common causes are obstructive sleep apnea (diagnosed by polysomnography), renal artery stenosis (diagnosed by renal duplex ultrasound or, preferentially, by CTA or MRA), and renal parenchymal disease. Uncommon causes of RH include pheochromocytoma (diagnosed by urinary or plasma metanephrine + normetanephrine, followed by imaging including total-body CTA or, preferentially, MRA), Cushing's disease, hyperparathyroidism, aortic coarctation, and intracranial tumor [Calhoun DA et al. Circulation 2008]. Screening for secondary hypertension also allows the adaptation of treatment regimens (eg, for low-renin hypertension) and to assess, if needed, the feasibility of device-based therapy including RDN or baroreceptor stimulation, which are still in the process of evaluation.
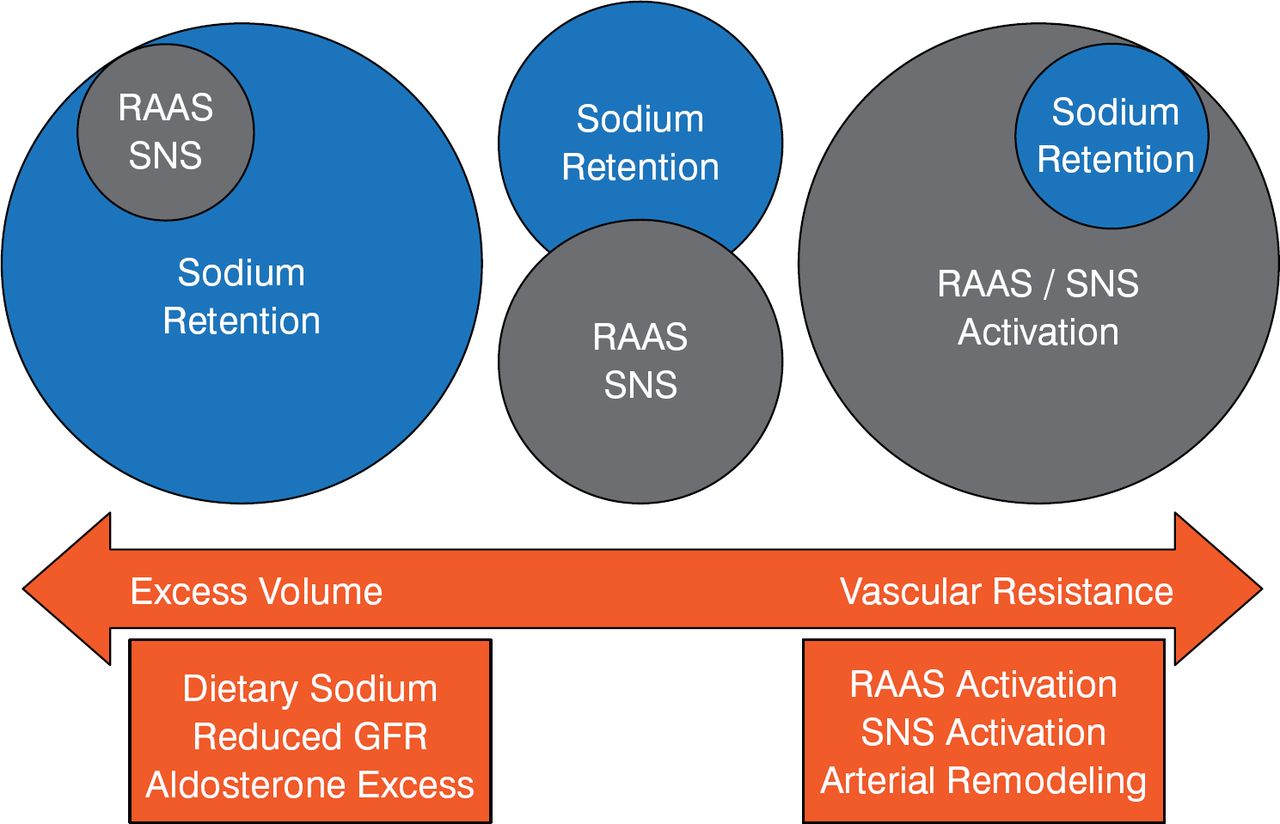
The pharmacologic treatment of true RH has been poorly studied, and the clinical evidence to guide treatment is clearly suboptimal, stated Bryan Williams, MD, University College London, London, United Kingdom. Drug treatment can be guided by the pathophysiologic basis of RH, that is, whether the phenotype is excess sodium retention, including excess aldosterone production, in which patients have excess volume, or renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system activation, in which patients have increased vascular resistance; diuretics are recommended for the former and RAAS blockers for the latter (Figure 1).

Pathophysiologic Approach to Drug Treatment of Resistant Hypertension
GFR=glomerular filtration rate; RAAS=renin-angiotensin-aldosterone system; SNS=sympathetic nervous system.
The predominant pathophysiologic cause of RH appears to be excess sodium retention, stated Prof. Williams, as shown by the nearly 67% of patients with RH who have low plasma renin activity despite being on treatment that should raise this level [Eide IK et al. J Hypertens 2004].
In patients with excess sodium retention resistant to diuretic therapy, additional approaches include a higher dose thiazide-type diuretic, adding low-dose spironolactone or eplerenone, or adding amiloride. In patients resistant to RAAS blocker therapy, an α-blocker or β-blocker can be added. Prof. Williams stated that the evidence for low-dose spironolactone (25 mg/day) is based on small post hoc analyses or observational studies showing that it lowers BP, but there are no data on clinical outcomes; the data are reviewed in the hypertension clinical practice guidelines of the National Institute for Health Care and Excellence [Krause T et al. BMJ 2011].
The recommendations from the ESH/ESC Guidelines for treating RH are based on evidence from subgroups of large-scale trials or observational studies. In patients on ≥3 AH drugs, including a diuretic, a good response has been reported with low-dose spironolactone or eplerenone, the a1 blocker doxazosin, a further increase in the diuretic dose, or replacing thiazides or chlorthalidone with a loop diuretic if renal function is impaired [Mancia G et al. J Hypertens 2013].
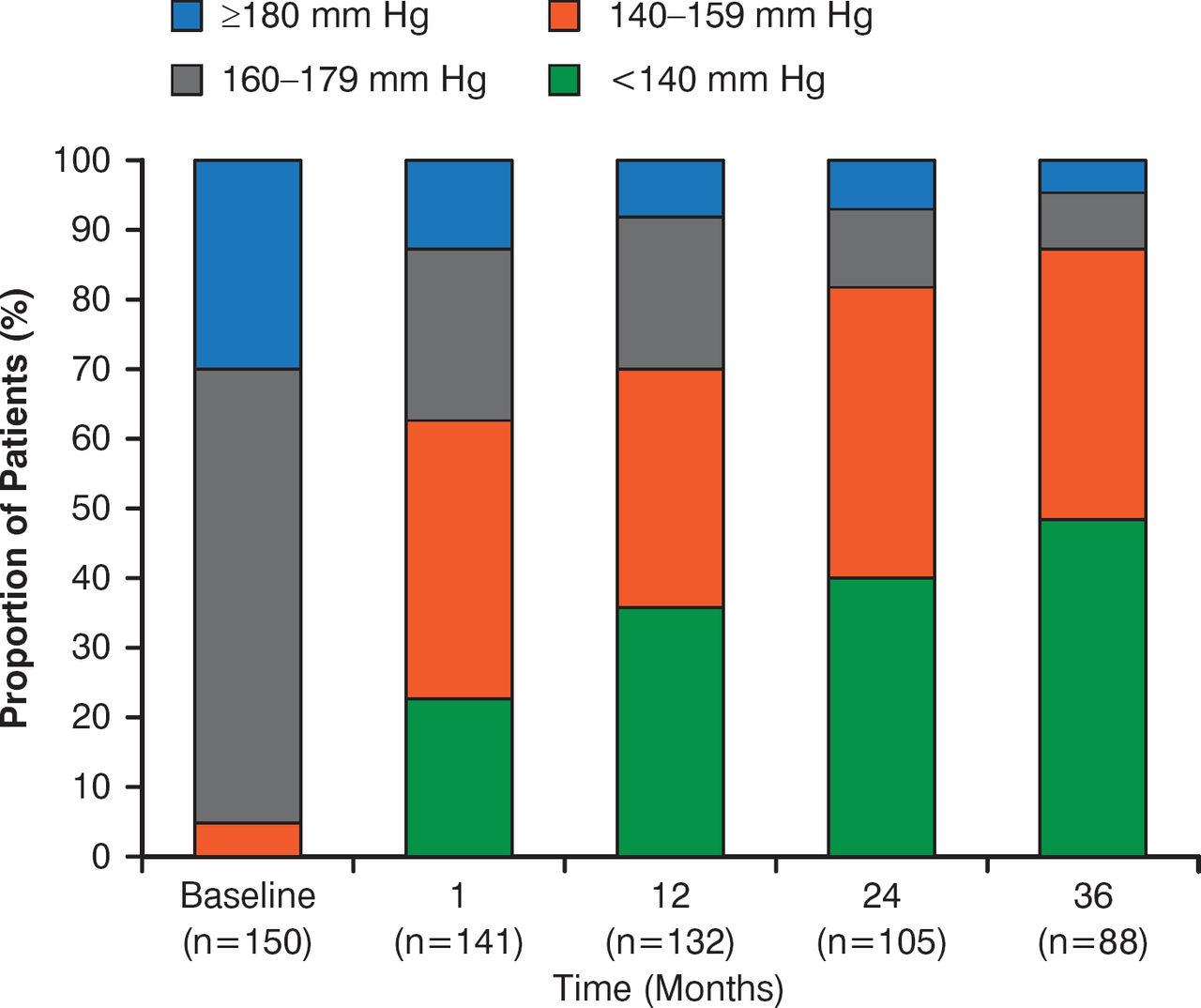
Markus Schlaich, MD, Baker Heart and Diabetes Institute, Melbourne, Australia, reviewed the 3-year results in 88 patients from the randomized, sham-controlled, open-label SYMPLICITY HTN-1 study of percutaneous RDN [Krum H et al. Lancet 2014]. The study patients had a mean age of 57 years, 42% were women, and 28% had diabetes. The mean estimated glomerular filtration rate was 85 mL/min/1.73 m2, and mean BP was 175/98 mm Hg at baseline.
The substantial, significant reduction in OBP was sustained at Year 3 (–32/14 mm Hg, p<0.01), without a change in the number of AH drugs. The proportion of patients with controlled BP increased progressively over 3 years, with about 93% having 10% improvements (Figure 2).

Distribution of Changes in Systolic Blood Pressure
GFR=glomerular filtration rate; RAAS=renin-angiotensin-aldosterone system; SNS=sympathetic nervous system.
Reproduced with permission from Elsevier from Krum H, Schlaich MP, Sobotka PA, et al. Percutaneous renal denervation in patients with treatment-resistant hypertension: final 3-year report of the Symplicity HTN-1 study. Lancet 2014;383(9917):622–629.
The treatment effect was consistent across subgroups (age, diabetes status, baseline renal function), and the increase in responder rates indicates that some patients respond late to RDN and that there was no loss of treatment effect at 3 years. Because the study patients were at high cardiovascular risk, the results are highly relevant, Dr. Schlaich noted. The procedure was safe, with no major adverse consequences.
Although the open-label experience with RDN appeared encouraging, enthusiasm has been tempered by the neutral results of the blinded SYMPLICITY HTN-3 trial. These results demonstrate the importance of blinded, appropriately controlled trials and the need for definitive evidence of benefit before the widespread adoption of novel interventions. Additional studies are needed to define if there is a benefit of RDN and which patients are most appropriate for this therapy.
Prof. Schlaich stated that regardless of the role RDN eventually plays in treating RH, it has stimulated new clinical and research interest in RH, and hopefully additional clinical trials will be conducted.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.