

Summary
The Nurse-led Intervention for Less Chronic Heart Failure study [NIL-CHF], a randomized controlled trial, has provided evidence that nurse-led care confers greater benefit to heart failure (HF) patients in terms of reduced time in emergency care and improved longer-term cardiac recovery.
- Heart Failure
- Cardiology Clinical Trials
- Heart Failure
- Cardiology & Cardiovascular Medicine
- Cardiology Clinical Trials
The Nurse-led Intervention for Less Chronic Heart Failure study [NIL-CHF], a randomized controlled trial, has provided evidence that nurse-led care confers greater benefit to heart failure (HF) patients in terms of reduced time in emergency care and improved longer-term cardiac recovery. The results of this study were presented by Simon Stewart, MD, Baker IDI Heart & Diabetes Institute, Melbourne, Australia.
Prevention of chronic HF (CHF) has only recently been studied [Ledwidge M et al. JAMA 2013]. Nurseled care may have potential benefit in reducing hospital admissions due to CHF [Pearson S et al. Arch Intern Med 2006]. The NIL-CHF trial explored the influence of nurseled management of patients with cardiovascular disease or a history of CHF on hospital admissions for CHF and all-cause mortality over a mean follow-up of 4.3 years (range, 41 to 66 months). The study was designed to create and test a program of care that cost-effectively prevents the development of CHF in at-risk patients without CHF.
Patients aged 45 years or older who had been admitted with a diagnosis of any cardiovascular condition except CHF were enrolled in this single-center study. Patients with CHF, as confirmed using echocardiography, or those who were subsequently re-admitted within 35 days for treatment of CHF were excluded. The primary end point was being event free after admission or all-cause mortality. Heart function was assessed (recovered, stable, or worse) 3 years after admission using echocardiography. Hospitalization rate and length of stay, all episodes of HF, emergency care, and any related cardiovascular events were recorded.
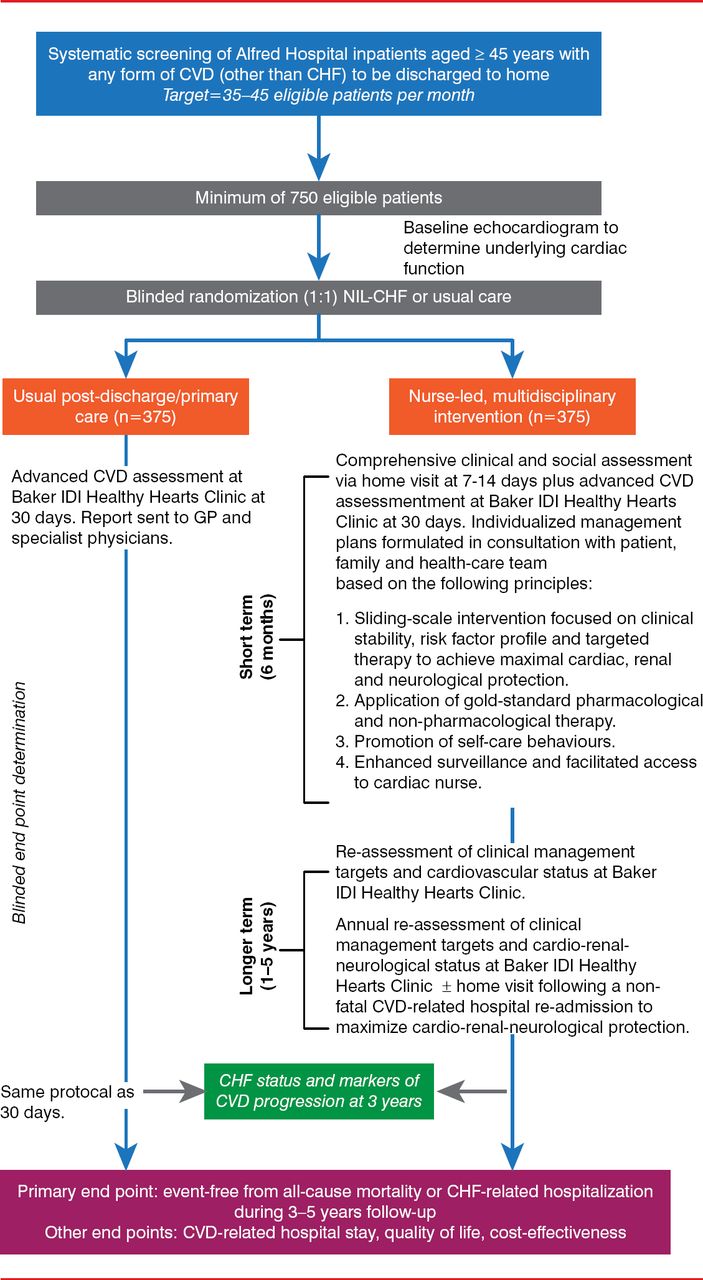
Patients were blindly randomized into usual-care or nurse-led clinical management, as described previously (Figure 1) [Carrington MJ & Stewart S. Eur J Heart Fail 2010]. The interventions included short- to medium-term support outside of the hospital (6 months) or longer-term support after the index hospital stay (18 months and 3 years). Support included telephone coaching and home visits, which were arranged based on the patients' clinical stability and their risk profile.

Study Design
Reproduced from Carrington MJ and Stewart S. Bridging the gap in heart failure prevention: rationale and design of the Nurse-led Intervention for Less Chronic Heart Failure (NIL-CHF) Study. Eur J Heart Fail 2010;12(1):82–88. With permission from John Wiley & Sons, Inc.
The study identified 5100 high-risk people with cardiovascular disease who had been discharged. Of these, 1059 were eligible for inclusion and 624 were randomized to usual post-discharge care (n=314) or nurse-led home- and clinic-based care (n=310). In total, 611 subjects (standard group, n=310; nurse-led group, n=301) were followed up with for a mean of 1561±240 and 1541±257 days, respectively.
The mean age of the cohort was 66±11 years, and the majority (71%) was male. Of the cohort, 62% were hypertensive; 70% were abdominally obese; 70% had coronary artery disease; 12.4% had asymptomatic left ventricular systolic dysfunction, 56% had asymptomatic HF with preserved ejection fraction, 13% had both cardiac conditions, and 18% had normal function; 83% were receiving antiplatelet therapy, 73% were receiving statin therapy, 71% were receiving angiotensin-converting-enzyme inhibitor or angiotensin receptor blocker, and 52% were receiving β-blockers.
There were 2507 hospital episodes representing 9847 days. Excluding same-day and emergency procedures, there were 827 all-cause admissions and 7824 days of hospitalization (median, 4.0 days; interquartile range, 3.0 to 9.0 days). Cardiovascular-related events included heart disease (n=455), musculoskeletal disease (n=385, of which 178 patients had chest pain), other cardiovascular disease (n=72), peripheral arterial disease (n=64), stroke or transient ischemic attack (n=40), and diabetes (n=22).
At the 3-year time point, there was no significant difference between the nurse-led care group and the usual care group relative to de novo hospitalization for heart failure (p=0.53) or death from any cause (p=0.797; primary end point comparison, p=0.493). More NIL-CHF cases showed reversal and recovery with respect to baseline left ventricular hypertrophy versus normal (39% vs 25%; p=0.047), initial left ventricular systolic dysfunction or HF with preserved ejection fraction versus normal (23% vs 16%; p=0.063), or any cardiac condition versus normal (36% vs 25%; p=0.011; OR, 1.35; 95% CI, 1.04 to 1.76). The nurse-led care produced improvements in many hospitalization-related parameters; however, only the number of emergency hospitalizations reached statistical significance (Table 1).
Hospital Admissions and Stay
Study limitations included the single-center design (albeit, an expert tertiary care center) and an open-label design. Nevertheless, the data show the promise of the nurse-led approach in the treatment of patients with CHF and support the further investigation of this strategy.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.