

Summary
In advanced esophageal cancer, 90% of patients have dysphagia as their predominant symptom. Although chemotherapy has demonstrated benefits in curing esophageal cancer, the only data on appropriate palliative treatment are from small, retrospective trials. The Advanced Oesophageal Cancer Study to Compare Quality of Life and Palliation of Dysphagia [NCT00193882] aims to establish effective and minimally toxic treatments for relief of dysphagia in advanced esophageal cancer and to determine the effects of common cancer treatments on quality of life.
- Radiation Therapy
- Oncology Clinical Trials
- Gastrointestinal Cancers
- Radiology
- Radiation Therapy
- Oncology Clinical Trials
- Oncology
- Gastrointestinal Cancers
- Radiology
While much focus is on exciting advancements in the cure of cancer, there is a group of patients who cannot be cured and who need effective treatment with minimal toxicity for their predominant symptoms. In advanced esophageal cancer, 90% of patients have dysphagia as their predominant symptom. Although chemotherapy has demonstrated benefits in curing esophageal cancer, the only data on appropriate palliative treatment are from small, retrospective trials.
Michael G. Penniment, MD, MBA, Royal Adelaide Hospital, Adelaide, Australia, directed the Advanced Oesophageal Cancer Study to Compare Quality of Life and Palliation of Dysphagia [NCT00193882], the aims of which were to establish effective and minimally toxic treatments for relief of dysphagia in advanced esophageal cancer and to determine the effects of common cancer treatments on quality of life (QoL). The primary protocol end point of this randomized phase 3 trial was the relief of dysphagia, defined as improvement of ≥ 1 point on the 5-point Mellow scale for dysphagia 9 weeks after starting radiation therapy (RT) and maintained until week 13. A secondary end point was dysphagia progression-free survival (PFS), measured from randomization to the time of first progression of dysphagia, which was defined as an increase of ≥ 1 point on the Mellow scale, stricture requiring intervention, or death.
The 220 patients (median age, 65 years; range, 37–88 years) recruited for the study were nearly evenly divided between those from Australia and New Zealand and those from Canada and the United Kingdom. Of these, > 80% were men and almost 70% presented with adenocarcinoma vs squamous cell carcinoma. Patients in Australia and New Zealand received RT of 35 Gy in 15 fractions, whereas those in Canada and the United Kingdom received 30 Gy in 10 fractions. The 111 patients randomized to chemotherapy received 5-fluorouracil 800 mg/m2/day on days 1 to 4 and cisplatin at either 80 mg/m2 IV at day 1 or 20 mg/m2 on days 1 to 4. Toxicity was measuring using Common Terminology Criteria for Adverse Events v2, whereas QoL was graded using the OES-18 module of the European Organisation for Research and Treatment of Cancer QLQ30 questionnaire.
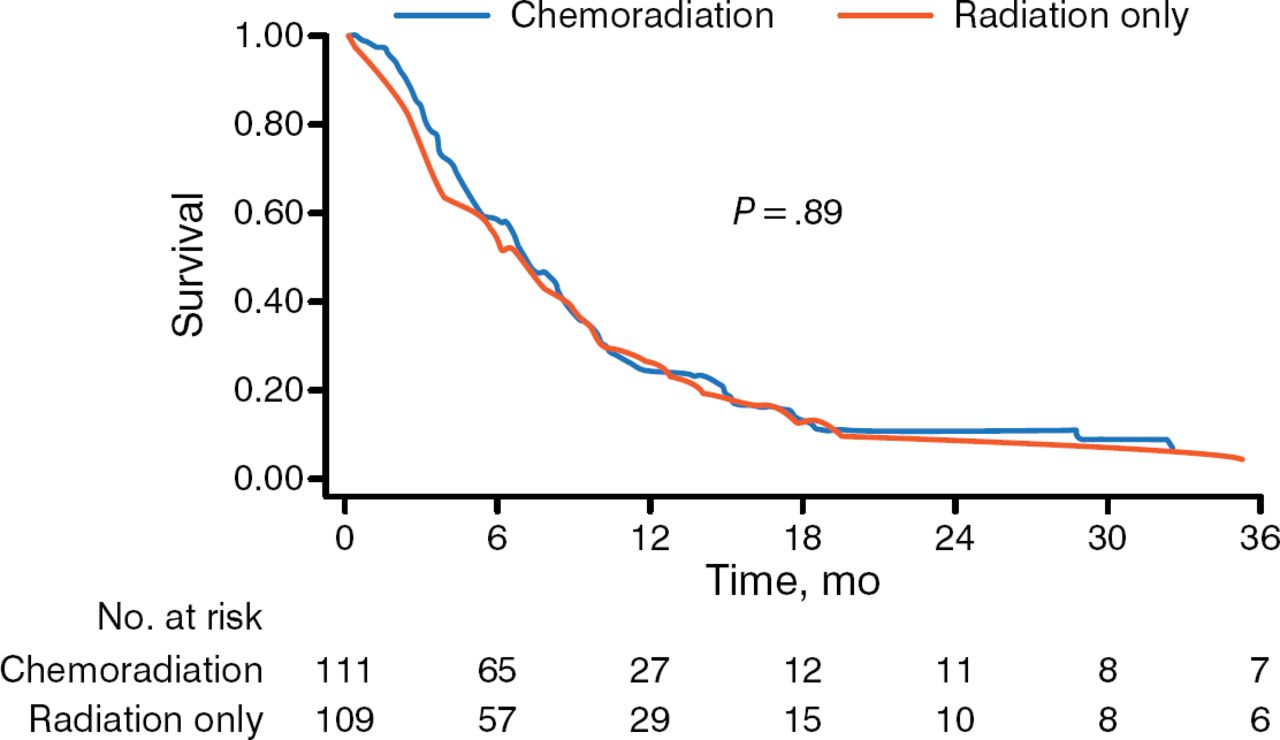
No statistically significant difference was seen in the 9-week dysphagia response or in the maintained response at week 13 between patients receiving RT alone and those receiving RT plus chemotherapy. There was also no significant difference between the 2 treatment arms for either dysphagia PFS or for overall survival (Figure 1). However, there was statistically significant increased toxicity (nausea and vomiting) in patients randomized to chemotherapy plus RT (P < .01). Despite increased toxicity, there was no significant difference between the arms on QoL analysis.

Overall Survival Comparing Radiotherapy With Chemoradiotherapy
Reproduced with permission from MG Penniment, MD, MBA.
In summary, in Dr Penniment's assessment, this trial must be considered negative because there was no significant improvement in dysphagia when chemotherapy was added to RT, and the trial was not powered to show equivalence. In addition, chemotherapy added to the RT did not improve QoL compared with RT alone. He concluded that treatment with RT alone should remain the standard of care for palliation of dysphagia in patients with advanced esophageal cancer.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.