

Summary
Low diastolic blood pressure (DBP) is associated with increased mortality in biologically older, frail elderly, whereas high DBP is associated with mortality in biologically younger, fit elderly. This article presents data from a population-based prospective study evaluating the effect of biological age on blood pressure (BP) control.
- Cardiology Clinical Trials
- Hypertensive Disease
- Cardiology Clinical Trials
- Hypertensive Disease
- Cardiology
Low diastolic blood pressure (DBP) is associated with increased mortality in biologically older, frail elderly, whereas high DBP is associated with mortality in biologically younger, fit elderly. Majon Muller, Leiden University Medical Center, Leiden, The Netherlands, presented data from a population-based prospective study evaluating the effect of biological age on blood pressure (BP) control.
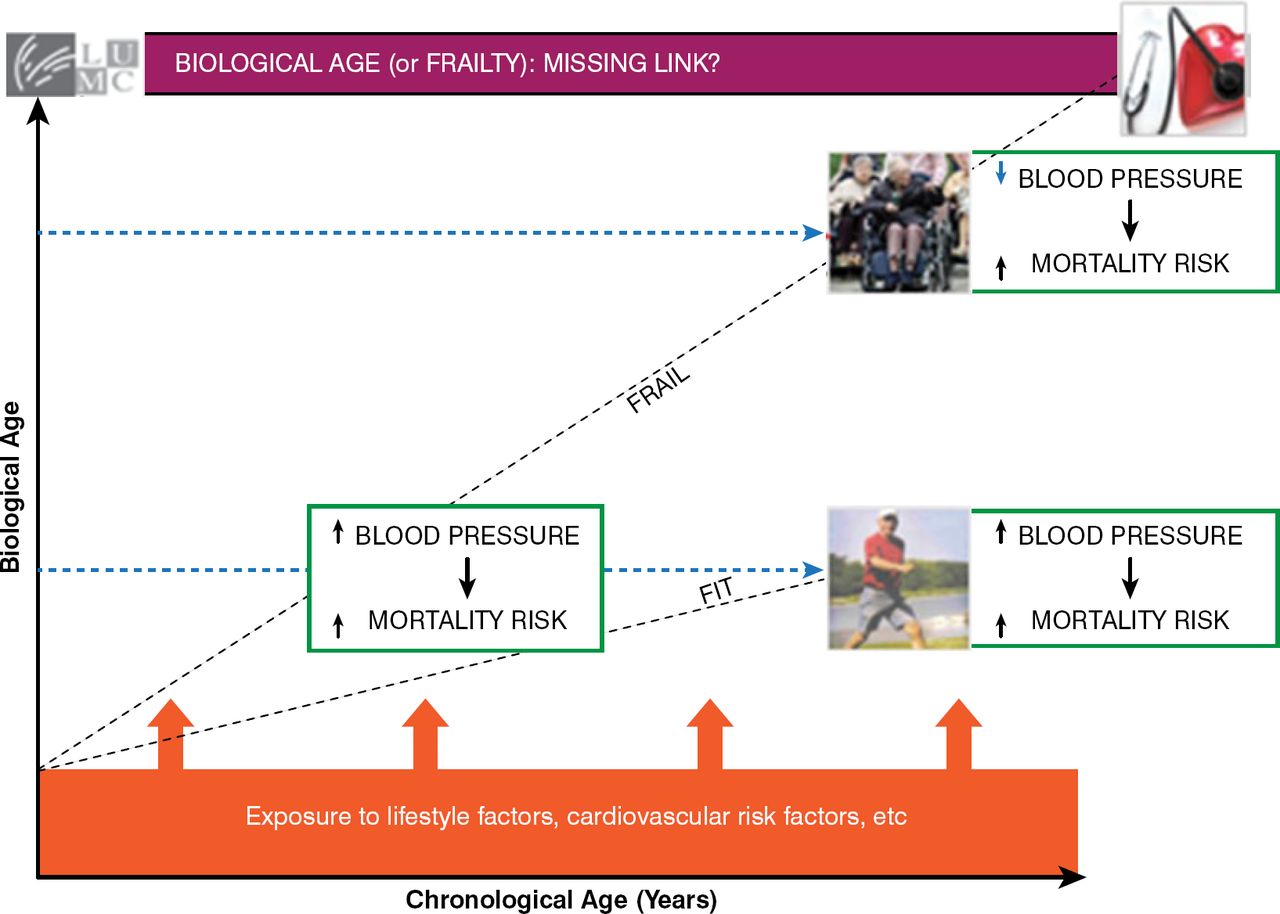
It is well known that high BP has been associated with an increased mortality risk [Lewington S et al. Lancet 2002]. However, this does not appear to hold true for patients who are very old or frail; in this population, lower BP has been associated with a greater risk of mortality (Figure 1) [Poortvliet RK et al. J Hyperten 2012; van Bemmel T et al. J Hypertens 2006; Hakala SM et al. Eur Heart J 1997]. It has been suggested that it is biological age, rather than chronologic age, that should be used to determine the effect of BP on mortality risk [Muller M et al. Hypertension 2014; Odden MC et al. Arch Int Med 2012]. The purpose of this study was to determine if physical and cognitive function can be used as indicators of biological age, which could elucidate the apparent complicated relation between BP and mortality in older populations.

Blood Pressure and the Risk of Mortality in the Fit Versus the Frail
Reproduced with permission from M Muller, MD.
In the population-based Longitudinal Aging Study Amsterdam, systolic BP (SBP) and DBP were related to mortality risk in 1466 older patients (mean age, 76 years) over 15 years of follow-up (mean follow-up, 11 years). The primary outcome was all-cause mortality, which was assessed with Cox regression analysis that adjusted for age, sex, cardiovascular risk factors, and cardiovascular disease. Biological age was measured by gait speed with the 6-meter walking test, and cognitive function was measured by the Mini—Mental State Examination (MMSE). Patients could achieve a biological age combination score of up to 4 points: 0 points for a gate speed of ≥0.8 m/s, 1 for <0.8 m/s, and 2 if the test could not be completed, as well as 0 points for achieving an MMSE score of >28, 1 for 27 to 28, and 2 for ≤26.
In the study, 49% of patients were men; 8% had diabetes; and 37% had cardiovascular disease. Mean (interquartile range) SBP and DBP were 151 mm Hg (134 to 170) and 82 mm Hg (74 to 91), respectively. In addition, 41% of patients were classified as “fit” (combination score of 0 or 1) and 59% as “frail” (combination score of 2 to 4).
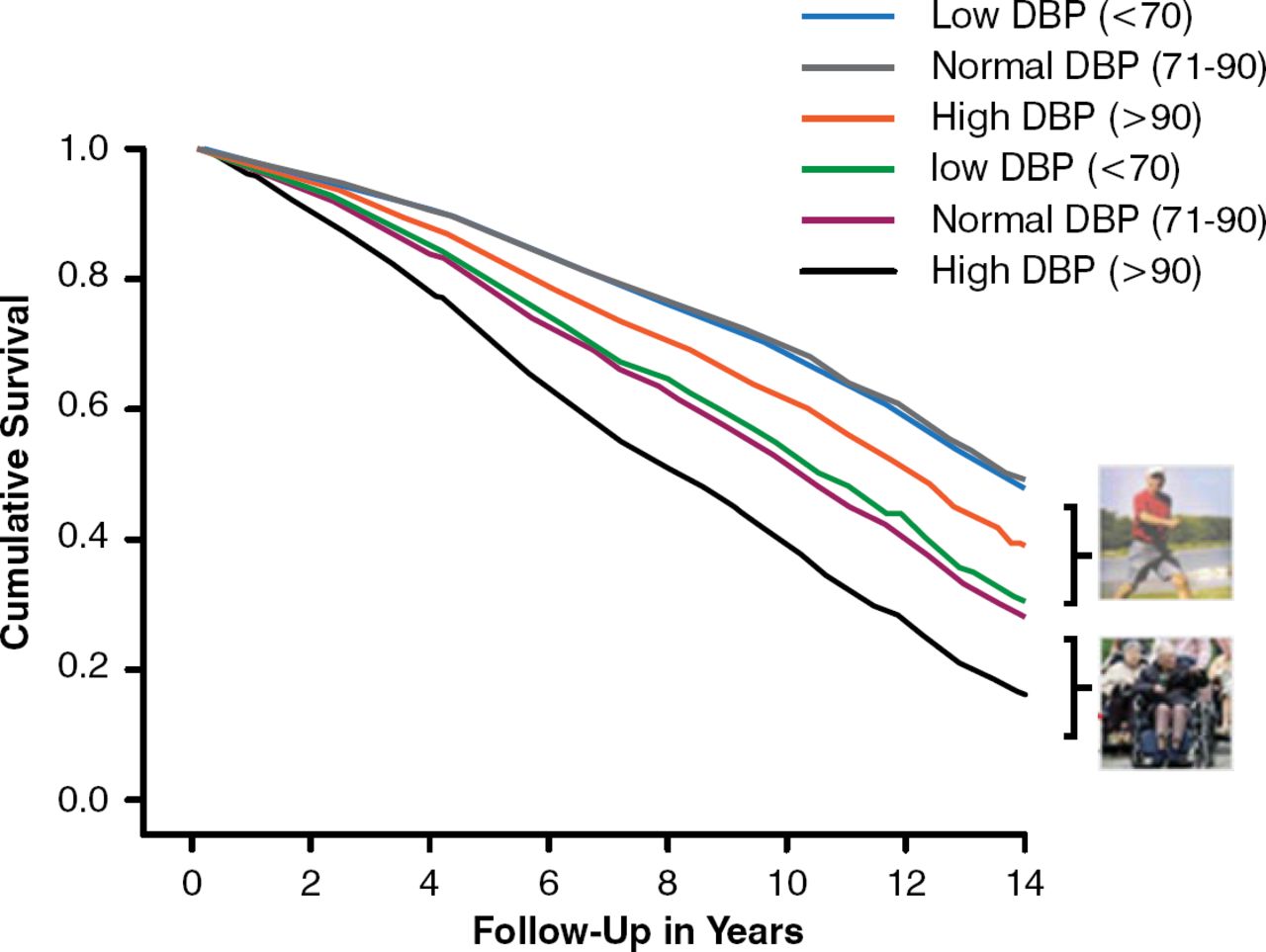
Compared with normal DBP (71 to 90 mm Hg), low DBP (≤70 mm Hg) was significantly associated with an increased mortality risk in frail, or biologically old, patients (HR, 1.5; 95% CI, 1.2 to 1.8) (Figure 2). In contrast, high DBP was associated with increased mortality risk in fit, or biologically younger, patients (HR, 1.5; 95% CI, 1.1 to 1.9; trend p=0.01). SBP was not associated with mortality.

Effect of Biological Age on Mortality Risk Stratified by Diastolic Blood Pressure
DBP=diastolic blood pressure.
Reproduced with permission from M Muller, MD.
Dr. Muller concluded that we need to refine our approach to thinking about optimal BP levels and that data from this study support the use of using markers of biological age to improve our understanding of the association between BP in late life and clinical outcomes.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.