

Summary
The Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation [COURAGE] trial evaluated percutaneous coronary intervention (PCI) as an initial management strategy in patients with stable coronary artery disease. Patients were randomly assigned to treatment with PCI in addition to medical therapy (n=1149) or medical therapy alone (n=1138). In the primary analysis, PCI did not reduce the risk of death or nonfatal myocardial infarction [Boden WE et al. N Engl J Med 2007].
- coronary artery disease
- interventional techniques & devices clinical trials
The COURAGE (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation) trial evaluated percutaneous coronary intervention (PCI) as an initial management strategy in patients with stable coronary artery disease (CAD). Patients were randomly assigned to treatment with PCI in addition to medical therapy (n=1149) or medical therapy alone (n=1138). In the primary analysis, PCI did not reduce the risk of death or nonfatal myocardial infarction (MI) [Boden WE et al. N Engl J Med 2007]. In this session, presenters discussed lessons from the COURAGE (NCT00007657) trial.
Optimal Medical Therapy For Most Patients
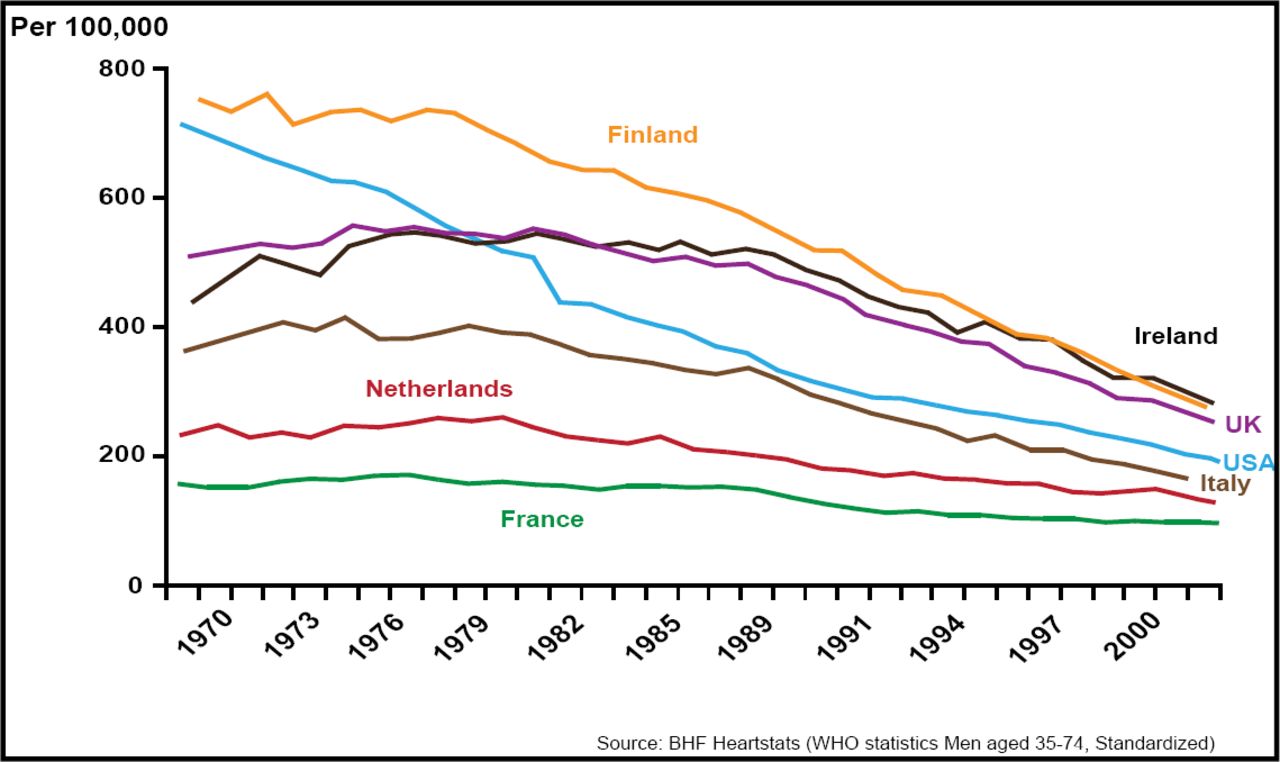
William E. Boden, MD, University of Buffalo, Buffalo, NY, argued in support of medical therapy as the initial choice in chronic stable angina. In 2007, Ford and colleagues described trends in cardiovascular mortality between 1980 and 2000 in the US [Ford ES et al. N Engl J Med 2007]. During this time period, the age-adjusted death rate for coronary heart disease (CHD) decreased by approximately half. As a result of the decreased mortality rate, there were 341,745 fewer deaths from CHD in 2000 versus 1980. The decreasing mortality that was observed in the US mirrors trends that have been observed worldwide (Figure 1).

International Trends in CHD Mortality, 1968–2003.
In the US study, researchers evaluated the causes of improved survival. They attributed 47% of the decline in mortality to the use of evidence-based medical therapies, including statins, angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, and other drug classes. An additional 44% of the decrease was due to positive changes in risk factors, such as decreased cholesterol levels, lower blood pressure, less smoking, and an increase in physical activity.
Only 5% of the increase in CHD-related survival was attributed to revascularization procedures for chronic stable angina. Specifically, PCI was responsible for only 1.3% of the improved survival that was observed between 1980 and 2000. “Although routine PCI provides some advantages in angina, they are numerically small, are not durable, and are achieved only at an unattractive cost for chronic disease management,” Dr. Boden said.
In summary, Dr. Boden said that aggressive medical therapy without initial PCI can be implemented safely in patients with stable CAD. Starting treatment with optimal medical therapy incurs no disadvantage with respect to death, MI, acute coronary syndrome, or revascularization, he concluded.
Identifying Patients For Revascularization
Marc E. Shelton, MD, Prairie Heart Institute, Springfield, IL, discussed strategies for identifying patients who are most likely to benefit from PCI. Among patients with chronic stable angina, the goals of PCI are to decrease symptoms, relieve ischemia, and reduce the need for subsequent procedures. However, PCI does not reduce the risk of death or MI in aggregate groups of patients with chronic stable angina and should not be used with these goals primarily in mind, Dr. Shelton said.
When considering the potential utility of PCI in specific patients, it is important to consider the extent of ischemia. In 2003, Hachamovitch and colleagues showed that revascularization has a greater survival benefit compared with medical therapy in patients with moderate to large amounts of inducible ischemia [Hachamovitch R et al. Circulation 2003]. The survival benefit of revascularization over medical therapy was seen in patients in whom more than 10% of the myocardium was at risk.
Dr. Shelton also emphasized the importance of medication adherence, whether patients are treated with optimal medical therapy or revascularization. Currently, only 40% of patients with CAD adhere to statin therapy after 2 years, and 1 in 7 patients who receive a drug-eluting stent does not continue antiplatelet therapy for 30 days following the procedure [Jackevicius CA et al. Circulation 2008; Spertus JA, et al. Circulation 2006].
In conclusion, in patients with chronic stable angina, Dr. Shelton suggested that PCI should be reserved for patients who have failed optimal medical therapy. In particular, patients who have significant myocardial risk areas and who are likely to be compliant with dual antiplatelet therapy are ideal candidates, he said.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.