

Summary
Diabetes is the fourth or fifth leading cause of death in most high-income countries, and evidence indicates that it is an epidemic in many economically developing and newly industrialized nations [IDF Diabetes Atlas, 4th ed. International Diabetes Federation 2011]. This article discusses the disease and its epidemiology, health impact, and intervention measures from a Caribbean perspective.
- Prevention & Screening
- Diabetes Mellitus
Diabetes is the fourth or fifth leading cause of death in most high-income countries, and evidence indicates that it is an epidemic in many economically developing and newly industrialized nations [IDF Diabetes Atlas, 4th ed. International Diabetes Federation 2011]. Hafeezul Mohammed, MD, FRCP, FACP, FACC, University of the West Indies, discussed the disease and its epidemiology, health impact, and intervention measures from a Caribbean perspective.
Diabetes
Type 1 diabetes is caused by an autoimmune reaction that destroys insulin-producing cells. The reason this occurs is not fully understood. While the disease can affect individuals of any age, it usually occurs in children or young adults. Type I diabetics require daily insulin injections, or they can suffer serious complications, including death [IDF Diabetes Atlas, 4th ed. International Diabetes Federation, 2011].
Type 2 diabetes is characterized by insulin resistance and relative insulin deficiency and accounts for at least 90% of all cases of the disease. It is usually diagnosed after the age of 40 years but can be identified earlier, especially in populations with high prevalence. Type 2 diabetes can remain undetected for many years, and the diagnosis is often made from associated complications or incidentally through abnormal blood or urine glucose tests [IDF Diabetes Atlas, 4th ed. International Diabetes Federation, 2011].
Often, type 2 diabetes is associated with obesity, which can cause insulin resistance and lead to elevated blood glucose levels. Other factors that drive the increasing rates of diabetes include rapid cultural and social changes, aging populations, increasing urbanization, dietary changes, reduced physical activity, and other unhealthy behavioral patterns [World Health Organization. Prevention of diabetes mellitus. Report of a WHO Study Group. Geneva: World Health Organization; 1994. No. 844].
Prevalence
Approximately 285 million people worldwide, or 6.6% of those aged 20 to 79 years, had diabetes in 2010; some 70% lived in low- and middle-income countries. Without preventive programs, this number is expected to increase by more than 50% in the next 20 years. By 2030, it is estimated that approximately 438 million people, or 7.8% of the adult population, will have diabetes, with the largest increases in regions that are dominated by developing economies [IDF Diabetes Atlas 4th ed. International Diabetes Federation, 2011].
The Caribbean has the highest prevalence of chronic noncommunicable diseases in the region of the Americas [Alafia Samuels T, Fraser H. Rev Panam Salud Publica 2010]. Diabetes mortality in Trinidad and Tobago and in Saint Vincent and the Grenadines is 6-fold higher than in North America (United States and Canada), and cardiovascular disease (CVD) mortality rates in Trinidad and Tobago, Guyana, and Suriname are 84%, 62%, and 56% higher, respectively, than in North America [Alafia Samuels T, Fraser H. Rev Panam Salud Publica 2010]. In Barbados, the prevalence and mortality rate of diabetes-related lower extremity amputations are among the highest in the world [Hennis AJ et al. Diabetes Care 2004; Hambleton IR et al. Diabetes Care 2009].
According to Dr. Mohammad, the overall prevalence of diabetes in the Caribbean is 9% versus a global rate of 6.4%. The figure for Trinidad and Tobago is 11.4%; for Jamaica, it is 10.2%; and for Barbados, 9.2% [IDF Diabetes Atlas, 4th ed. International Diabetes Federation, 2011].
Natural History of Diabetes and Complications
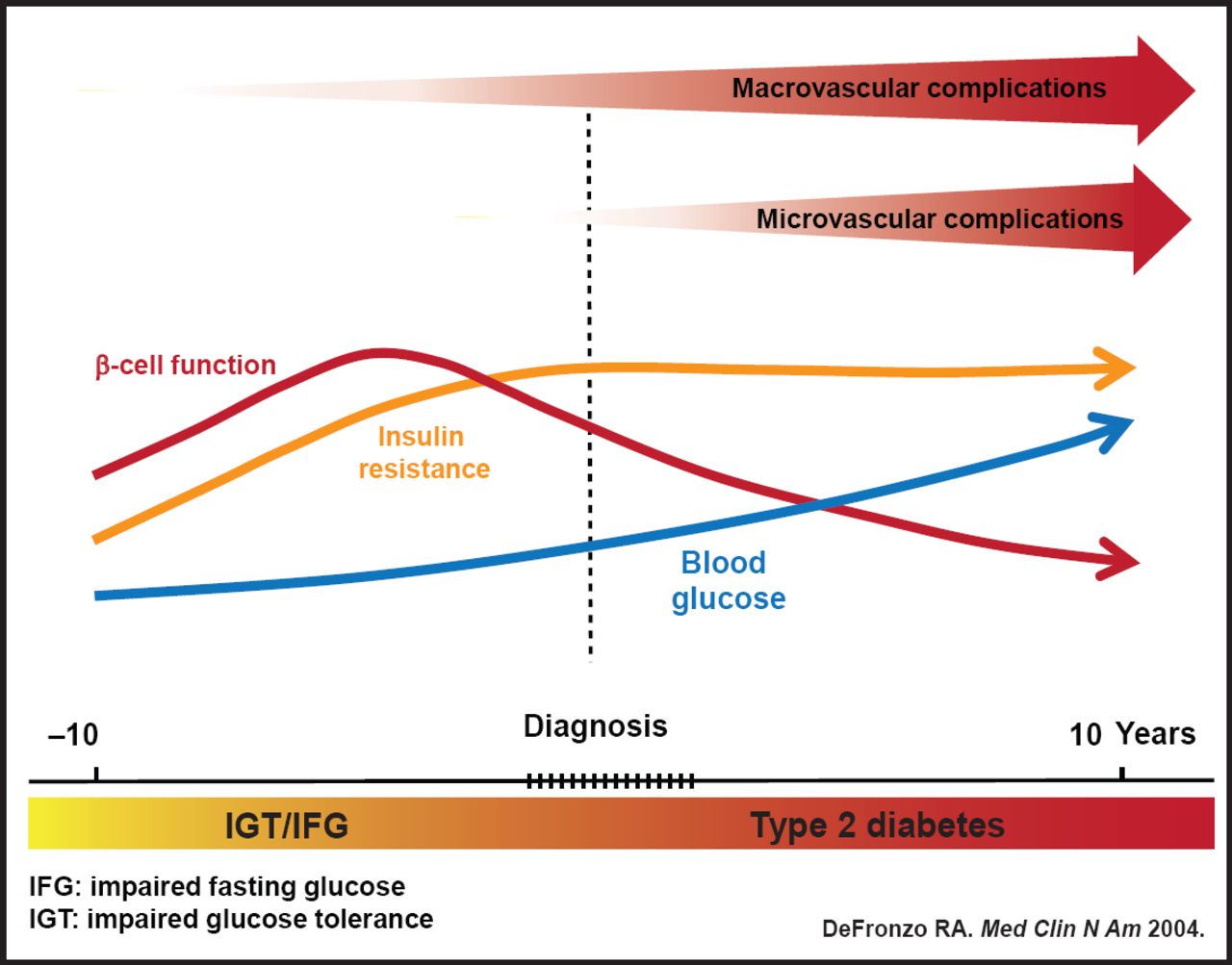
Type 2 diabetes is a progressive disease that is characterized by two fundamental defects: insulin resistance and β-cell dysfunction. It starts with normal glucose tolerance, insulin resistance, and compensatory hyperinsulinemia, with progression to impaired glucose tolerance (IGT) and overt diabetes (Figure 1) [deFronzo RA. Med Clin N Am 2004]. Chronic elevation of blood glucose, even when no symptoms are present, will eventually lead to tissue damage, with consequent, and often serious, disease. Evidence of micro- and macrovascular damage can be found in many organ systems, especially the kidneys, eyes, peripheral nerves, and vascular tree. Complications from diabetes are significant and sometimes fatal [deFronzo RA. Med Clin N Am 2004].

Natural History of Disease Progression.
Reproduced with permission from H. Mohammed, MD.
Cardiovascular Disease
CVD is the major cause of death in diabetes, accounting in most populations for 50% or more of all fatalities and much disability. The kinds of CVD that accompany diabetes include angina, myocardial infarction, stroke, peripheral artery disease, and congestive heart failure.
Over 4 years of follow-up, Hennis et al. found that among 4709 individuals aged 40 to 84 years and born in Barbados, the cumulative mortality among diabetics was 10.2%, with a 9% increase in 4-year mortality for each 1% increase in HbA1C. Overall, diabetics had a 42% higher risk of death compared with those who did not have the disease [Hennis A et al. Int J Epidemiol 2002].
According to Dr. Mohammad, the Jamaican Ministry of Health reported that diabetes accounted for 60 of every 100,000 deaths in 1999 and was the third leading cause of mortality. In 2004, it accounted for 70 of every 100,000 deaths and was the second leading cause of mortality. McDougal et al. found that diabetes-related mortality in 17 Caribbean countries increased 50% from 1981–1985 (40/100,000 to 60/100,000) [McDougal L. CAREC Surveillance Report 2006].
Complications
Diabetes is linked to diabetic retinopathy, the leading cause of blindness in working age adults [Fong DS et al. Diabetes Care 2003]. Other diabetes-related complications include diabetic nephropathy, the leading cause of end-stage renal disease [Molitch ME et al. Diabetes Care 2003]; stroke (a 2- to 4-fold increase in cardiovascular mortality and stroke) [Kannel WB et al. Am Heart J 1990]; and diabetic neuropathy, the leading cause of nontraumatic lower extremity amputations [Mayfield JA et al. Diabetes Care 2003].
Intervention
Treatments include lifestyle changes (diet and exercise) and medications. Current American Diabetes Association treatment targets call for HbA1C <7%; blood pressure <130/80 mm Hg; low-density lipoprotein cholesterol <100 mg/dL; high-density lipoprotein cholesterol in men >40 mg/dL and in women >50 mg/dL; and triglycerides <150 mg/dL [American Diabetes Association. Diabetes Care 2010].
The increasing prevalence of diabetes in the Caribbean represents a significant disease burden that is associated with serious microvascular and macrovascular complications. Early detection and risk factor interventions are crucial for successful prevention and management of the disease.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.