

Summary
Risk stratification tools are critical for classifying cardiovascular (CV) risk and guiding therapy, particularly in asymptomatic patients. In this session, experts discussed new data that support the use of noninvasive imaging modalities as adjuncts to traditional risk factors in CV risk assessment.
- Prevention & Screening
- Cardiac Imaging Techniques
- Imaging Modalities
Risk stratification tools are critical for classifying cardiovascular (CV) risk and guiding therapy, particularly in asymptomatic patients. In this session, experts discussed new data that support the use of noninvasive imaging modalities as adjuncts to traditional risk factors in CV risk assessment.
Pulse Wave Velocity
The 2010 American Heart Association (AHA) guideline for the assessment of CV risk in asymptomatic adults recommends against the routine measurement of arterial stiffness outside of research settings. In particular, the AHA concluded that there is no benefit to measuring pulse pressure or aortic pulse wave velocity (PWV) in asymptomatic adults [Greenland P et al. Circulation 2010]. More recent findings, however, suggest an emerging role for assessing PWV in clinical practice. Gary F. Mitchell, MD, Cardiovascular Engineering, Inc., Norwood, Massachusetts, USA, described new insights into the value of PWV in CV risk assessment.
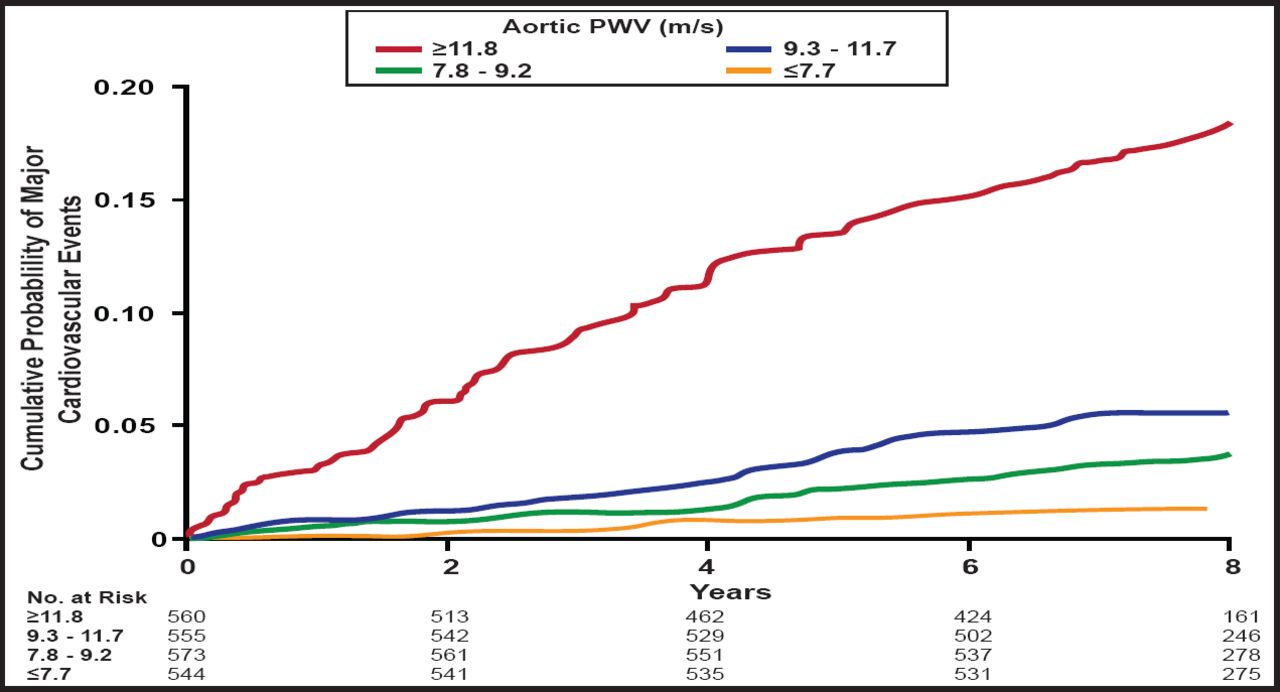
In 2010, Mitchell and colleagues were the first to describe the prognostic stratification, discrimination, and risk reclassification that were achieved by adding PWV to standard risk factors in the community setting [Mitchell GF et al. Circulation 2010]. In the study, investigators evaluated PWV, wave reflection, and central pulse pressure in 2232 participants in the Framingham Heart Study. After a median follow-up of 7.8 years, 6.8% of patients experienced a first major CV event, such as myocardial infarction (MI), unstable angina, heart failure (HF), or stroke. In models that adjusted for standard risk factors, higher aortic PWV at baseline was associated with a 48% increase in the risk of a CV event (HR, 1.48 per SD; 95% CI, 1.16 to 1.91; p=0.002). Patients in the highest quartile of PWV had more than 3-fold the cumulative risk of major CV events compared with those in the lowest quartile of PWV (HR Q4 vs Q1, 3.4; 95% CI, 1.4 to 8.3; p=0.008; Figure 1). By comparison, baseline wave reflection, central pulse pressure, and pulse pressure amplification values did not correlate with CV disease outcomes. Adding PWV to components of the standard Framingham Risk Score improved the predictive value of this risk factor model (p<0.05).

Carotid-Femoral PWV and CV Events in the Framingham Heart Study.
Copyright © 2011 American Heart Association. All rights reserved.
Which measure of PWV is preferred for widespread patient screening and risk assessment? The carotid-radial PWV captures muscular arterial PWV, while the carotid-femoral PWV provides a true assessment of aortic PWV. Carotid-femoral PWV clearly predicts CV outcomes and improves risk stratification beyond that provided by standard risk factor measures. Moreover, carotid-femoral PWV is noninvasive, reproducible, fast, and inexpensive. Future clinical guidelines may be revised to include carotid-femoral PWV as a routine measure of CV risk assessment, based on these data, Dr. Mitchell said.
Coronary Artery Calcification
Vulnerable atherosclerotic plaques are characterized by a large lipid core, a thin fibrous cap, inflammatory cell infiltration, and spotty calcification. Coronary artery calcium (CAC) screening with computed tomography (CT) scanning provides a noninvasive method for measuring the presence and degree of calcification within arterial walls. Paolo Raggi, MD, Emory University, Atlanta, Georgia, USA, described new insights into the interpretation of coronary calcium scores.
Higher CAC scores are associated with an increased risk of CV morbidity and mortality, whereas the absence of CAC reliably identifies low-risk patient groups. Adding the coronary calcium score to the Framingham Risk Score improves the predictive value of traditional risk factors for MI or CV death in patients without established CV disease [Greenland P et al. JAMA 2004]. Yet, current approaches to CAC scoring have important limitations; CAC scoring may not be uniformly informative for all patient groups. In the Multi-Ethnic Study of Atherosclerosis (MESA), black patients had significantly less CAC than Caucasian patients, and Hispanic patients had slightly less than Caucasians. Across all patient groups, Asian patients had the least amount of coronary calcification [Wang L et al. J Am Coll Cardiol 2006].
Advances in CAC screening technology may provide a more nuanced assessment of CV risk in diverse patient populations. Besides CAC, the presence of aortic and valvular calcification has also been shown to predict adverse CV events and be associated with characteristics of plaque vulnerability. Investigators from Hiroshima University in Hiroshima, Japan, examined the association of aortic valve calcification (AVC) and mitral annual calcification (MAC) to coronary atherosclerosis using 64-multidetector CT (MDCT). In the study of 322 patients, the combined presence of AVC and MAC strongly correlated with the presence and extent of coronary plaques that were identified by 64-MDCT. In a multivariate analysis, the combined presence of AVC and MAC was also associated with vulnerable characteristics of coronary plaque [Utsunomiya H et al. Atherosclerosis 2010].
Carotid Intima-Media Thickness
Carotid intima-media thickness (CIMT) is validated as a surrogate marker for atherosclerosis and atherosclerosis-related coronary heart disease (CHD) and stroke. Although CIMT is often used as a surrogate endpoint in clinical trials, its place in routine risk assessment remains unclear. Vijay Nambi, MD, Baylor College of Medicine, Houston, Texas, USA, discussed the evolving role of CIMT in CV risk assessment.
Adding CIMT to traditional risk factors significantly improved CV risk predication in the Atherosclerosis Risk in Communities (ARIC) Study [Nambi V et al. J Am Coll Cardiol 2010]. Despite its correlation with CV outcomes, CIMT has important limitations that are related to risk assessment. Serial CIMT measurements assume uniform thickness along the blood vessel. Changes in CIMT may preferentially reflect changes in media thickness, while most changes in atherosclerosis occur in the intima. Moreover, changes in CIMT are difficult to monitor in individual patients, with annual changes in the range of 0.01 mm.
Compared with all carotid artery segments (A-CIMT), assessing the common carotid artery intima-media thickness (CCA-IMT) is easier and more reliable. Several major studies recently assessed the utility of CCA-IMT as a predictor of CV risk. In a subanalysis of the ARIC Study, Dr. Nambi and colleagues demonstrated that adding CCA-IMT to traditional risk factors is comparable with adding A-CIMT and therefore is a reliable alternative to measuring A-CIMT for CV risk prediction [Nambi V et al. Eur Heart J 2011].
Polak and colleagues evaluated the predictive value of CCA-IMT in 2965 members of the Framingham Offspring Study cohort. Both A-CIMT and CCA-IMT correlated with CV outcomes, but only A-CIMT significantly improved the classification of CV risk compared with traditional risk factors, and its impact was marginal [Polak JF et al. N Engl J Med 2011]. The Three-City Study evaluated CCA-IMT in 5895 adults aged 65 to 85 years who were free from CHD at baseline. After a median follow-up of 6 years, the baseline CCA-IMT measurement did not improve risk prediction compared with traditional risk factors alone [Plichart M et al. Atherosclerosis 2011]. Therefore, the role for measuring CCA-IMT to assess CV risk prediction in clinical practice remains unclear.
CAC scoring has emerged as the most useful of the noninvasive imaging tests for reclassifying short-term CHD risk. Different imaging tests may be selected for different endpoints of interest, as needed. In particular, CIMT is the strongest predictor of stroke, while left ventricular mass strongly correlates with HF. Current guidelines focus on the use of imaging studies in intermediate-risk patients. Future studies will help determine the clinical utility of imaging in earlier and later phases of atherosclerotic disease.
- © 2011 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.