

Summary
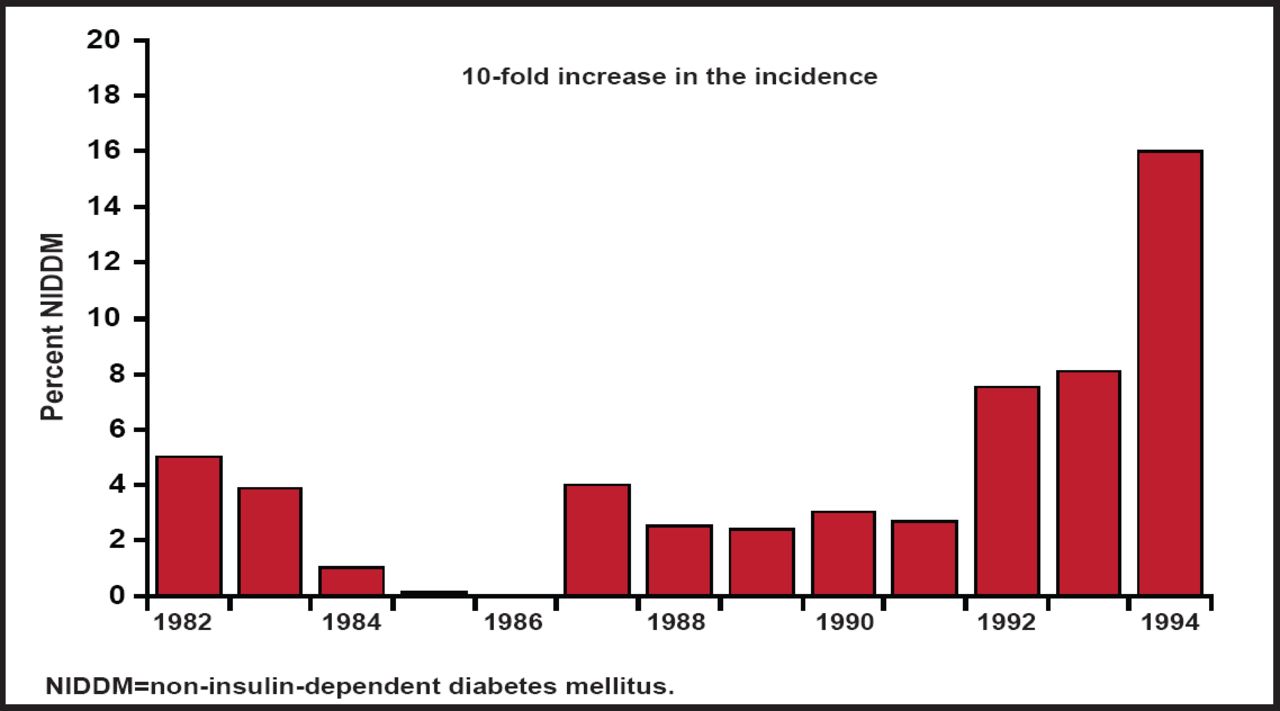
A study of the medical records of 1027 consecutive pediatric patients from birth to age 19 years found that the number with a new diagnosis of type 2 diabetes mellitus (T2DM) rose from approximately 4% before 1992 to 16% in 1994 [Pinhas-Hamiel O et al. J Pediatr 1996], and the trend has only accelerated over time.
- Prevention & Screening
- Diabetes Mellitus
A study of the medical records of 1027 consecutive pediatric patients from birth to age 19 years found that the number with a new diagnosis of type 2 diabetes mellitus (T2DM) rose from approximately 4% before 1992 to 16% in 1994 (Figure 1) [Pinhas-Hamiel O et al. J Pediatr 1996], and the trend has only accelerated over time. Silva Arslanian, MD, Children's Hospital of Pittsburgh, Pittsburgh, Pennsylvania, USA, discussed the presentation and management of T2DM in the young, including clinical characteristics, pathophysiology, risk factors, and treatments.

Ten-Fold Increase in the Incidence of T2DM Between 1982 and 1994 in a Pediatric Diabetes Clinic.
Reproduced with permission from S. Arslanian, MD.
According to Dr. Arslanian, the prevalence of T2DM in children is not yet epidemic but is increasing rapidly. In describing the clinical characteristics, she said that the disease is common in minorities, the age of diagnosis occurs between 12 and 14 years, and T2DM affects more females than males with body mass index from 29 to 38 kg/m2. Ketoacidosis affects between 5% and 53% of patients.
Recent data from the Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) cohort show similar findings. The cohort included various racial/ethnic groups with low socioeconomic status and a family history of diabetes; clinical and biochemical abnormalities and comorbidities were prevalent within 2 years of T2DM diagnosis [Copeland KC et al. J Clin Endocrinol Metab 2011].
Hyperglycemic hyperosmolar nonketotic coma (HHNK) can occur as a serious complication of borderline and unrecognized T2DM. Foutner et al. found that HHNK affected 3.7% of patients, with a mean serum osmolality 393 mOsm/L, glucose level of 88.4 mmol/L, and case fatality of 14.3% [Fourtner SH et al. Pediatr Diabetes 2005].
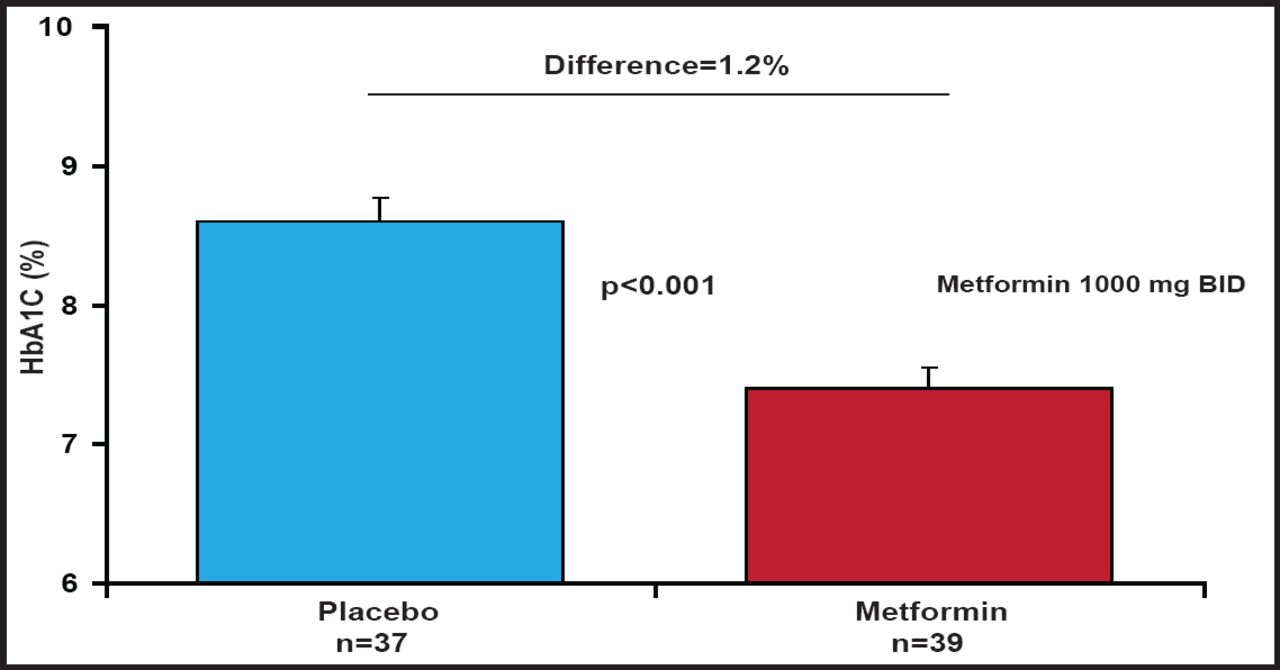
The TODAY study [The TODAY Study Group. Pediatr Diabetes 2007] showed that most youngsters can achieve satisfactory glycemic control when treated with metformin alone, following initial insulin therapy. In a randomized controlled trial, Jones et al. [Diabetes Care 2002] found that the adjusted mean change from baseline in fasting plasma glucose was −2.4 mmol/L (−42.9 mg/dL) for metformin compared with 1.2 mmol/L (+24.1 mg/dL) for placebo (p<0.001). Mean HbA1C vales, adjusted for baseline, were also significantly lower with metformin compared with placebo (7.5% vs 8.6%, respectively; p<0.001; Figure 2).
According to Dr. Arslanian, rosiglitazone, sulfonylureas, and bariatric surgery are not approved by the United States Food and Drug Administration for treatment of T2DM in pediatric patients. Even though youth with newly diagnosed T2DM respond to lifestyle change plus metformin (1000 mg BID; Figure 2), severe cases (with hyperglycemia, polyuria, polydipsia, weight loss, and ketonuria or ketoacidosis) call for insulin in combination with lifestyle change and metformin to rapidly control and correct the hyperglycemia and the metabolic derangements.

HbA1C at Week 16.
Reproduced with permission from S. Arslanian, MD.
In pediatric patients with newly diagnosed T2DM, glycemic control, as measured with HbA1C, improves with implementation of treatment and is maintained within the goal range for almost 2 years, after which there is gradual deterioration with increasing HbA1C levels. Unlike adults, children with T2DM require increasing insulin doses over a 4-year period, and ketoacidosis at diagnosis predicts greater β-cell decline over time [Levitt Katz LE et al. J Pediatr 2011].
Before the 1990s, it was rare for pediatric centers to have patients with T2DM. With the rapid rise in obesity, however, their presence has dramatically increased worldwide [The TODAY Study Group. Pediatr Diabetes 2007]. New treatments that are on the horizon include GLP-1R agonists, such as exenatide and liraglutide, and DPP-4 inhibitors, such as sitagliptin.
- © 2011 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.