

Summary
The sympathetic nervous system (SNS) has recently been hypothesized to play a key role in resistant hypertension. As a result, recent studies have explored renal artery denervation therapy as a potential treatment option for patients with resistant hypertension. This article discusses the current and future landscape of renal denervation therapy, as well as potential mechanisms by which increased sympathetic activity may result in effect blood pressure.
- Renal Disease
- Interventional Radiology
- Hypertension & Kidney Disease
- Hypertensive Disease
- Cardiology & Cardiovascular Medicine
- Renal Disease
- Interventional Radiology
- Hypertension & Kidney Disease
- Hypertensive Disease
The sympathetic nervous system (SNS) has recently been hypothesized to play a key role in resistant hypertension. As a result, recent studies have explored renal artery denervation therapy as a potential treatment option for patients with resistant hypertension. Mohammad I. Kurdi, MBBS, Al Takhassoussi Hospital, Riyadh, Saudi Arabia, presented the current and future landscape of renal denervation therapy.
Systemic hypertension is associated with major adverse cardiac and cerebral events and pharmacologic control of hypertension has been shown to reduce cardiovascular and cerebrovascular events. However, some patients continue to have poorly controlled hypertension despite multidrug therapy or have adverse drug events or contraindications to pharmacotherapy that prevent adequate control of hypertension. Interestingly, increased sympathetic tone, in part mediated by the kidneys, has been hypothesized as a potential mechanism in the pathophysiology of hypertension. Therefore, several recent studies sought to evaluate the benefit of therapies that inhibit the effects of the kidneys on the sympathetic nervous system in patients with resistant hypertension.
Although the results of an ongoing, large randomized, controlled trial are needed to confirm the efficacy and safety of renal denervation therapy, Prof. Kurdi stated that several smaller studies have demonstrated that surgical renal sympathectomy can result in improved blood pressure control. The potential benefits of renal denervation therapy may include decreased cardiac size, improved renal function, decrease incidence of headache, decreased precordial pain, and fewer cerebrovascular events.
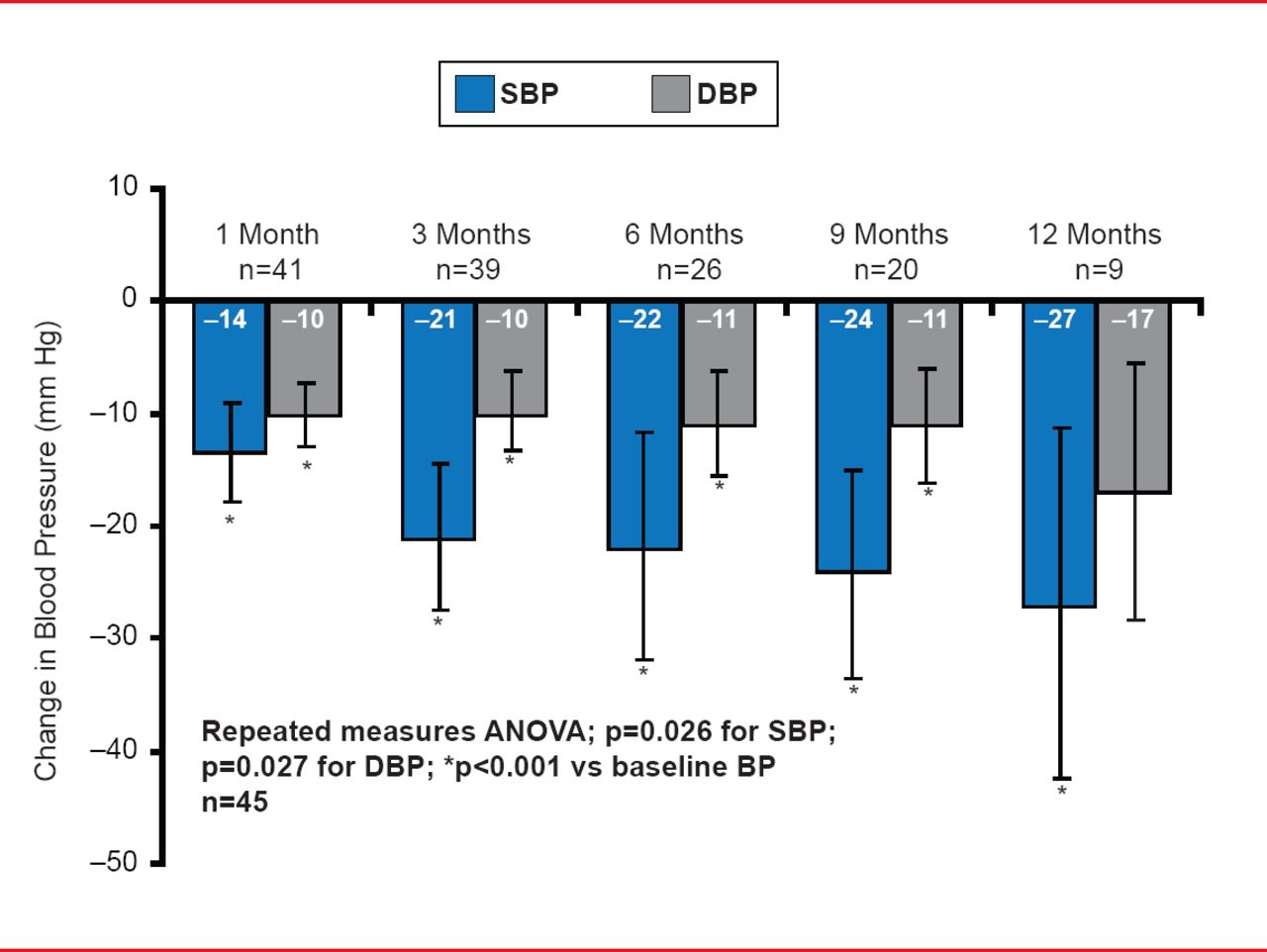
In the Catheter-Based Renal Sympathetic Denervation for Resistant Hypertension proof-of-principle trial [Symplicity HTN-1 Investigators; Krum H. Hypertension 2011], bilateral radiofrequency application to the renal arteries was evaluated in 45 patients with drug-resistant hypertension. Following renal artery angiography, patients received anticoagulation therapy and opioid analgesics for diffuse abdominal pain. An 8-French guide catheter was used via an 8-French femoral artery access and positioned in the renal arteries, with subsequent radiofrequency application. Patients experienced a significant decrease in systolic blood pressure of 14 mm Hg at 1 month and 27 mm Hg at 12 months. Diastolic blood pressure decreased by 10 mm Hg at 1 month and 17 mm Hg at 12 months. In addition, the antihypertensive medications were adjusted in 13 patients; 9 patients had a decrease in the number of antihypertensive medications while 4 patients had an increase. Importantly, even after adjusting for the 4 patients whose treatment was intensified, the blood pressure was significantly reduced. No response to renal denervation therapy occurred in 13% of patients.
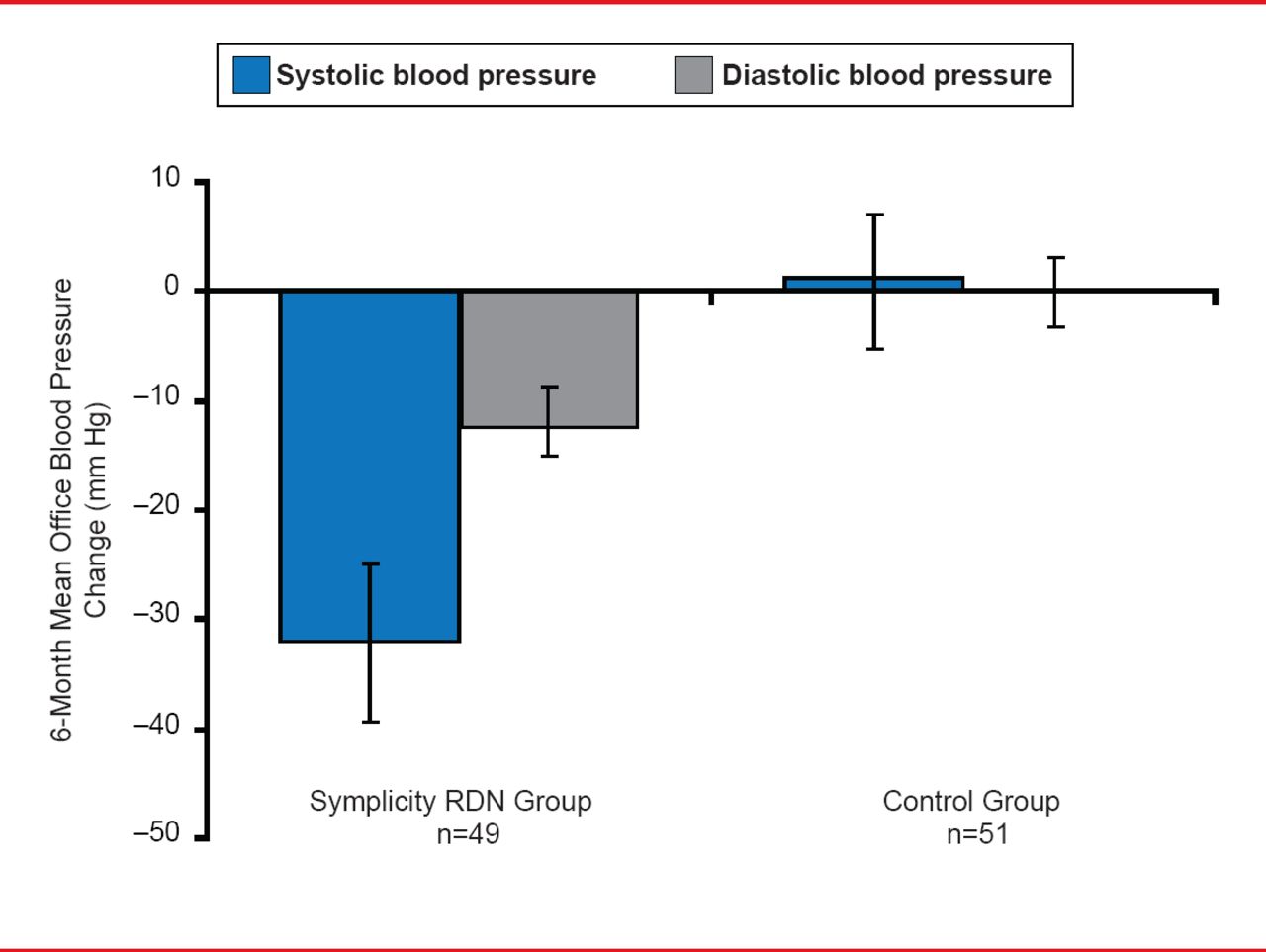
In the Renal Sympathetic Denervation in Patients With Treatment-Resistant Hypertension trial [Symplicity HTN-2 Investigators; Esler MD et al. Circulation 2012], 106 patients with resistant hypertension were randomized to receive catheter-based renal sympathectomy plus pharmacologic treatment or pharmacologic treatment only. Patients that received catheter-based therapy experienced a significantly greater blood pressure reduction from baseline compared with pharmacologic therapy only, with a mean blood pressure decrease of 33/11 mm Hg at 6 months' follow-up (p<0.0001; Figure 1). In addition, 84% of patients treated with renal sympathectomy experienced a blood pressure decline of at least 10 mm Hg compared with 35% of patients that received pharmacologic therapy only (p<0.001).
Prof. Kurdi explained the structure of several renal denervation systems. The Symplicity systems include the first-generation denervation system, a single-point ablation catheter that is manually rotated with 4 points of ablation, and the second generation denervation catheter with a spiral, helical-shaped wire with 4 simultaneous points of ablation. The EnligHTN System consists of a catheter with 4 electrodes placed in staggered positions in a basket configuration, each having a temperature and impedance sensor.

Mean Change in Blood Pressure Following Renal Denervation in the Symplicity HTN-2 Trial
Reproduced from Esler MD et al. Renal Sympathetic Denervation for Treatment of Drug-Resistant Hypertension: One-Year Results From the Symplicity HTN-2 Randomized, Controlled Trial. Circulation 2012;126(25):2976–2982. With permission from Lipincott, Williams and Wilkins.
Emerging renal sympathectomy systems are balloon-based and include the Covidien system, which has 8 ablation sites with water irrigation and a timing of 2 minutes; the Boston Scientific Balloon with 8 ablation points and a timing of 30 seconds; and the Cordis system. Prof. Kurdi suggested that renal sympathectomy should be evaluated in the treatment of other cardiovascular diseases including, heart failure and severe hypertension with end organ damage (eg, left ventricular hypertrophy, proteinuria, or retinopathy), since reduction in blood pressure in patients with these conditions may also improve cardiovascular outcomes.
Mahmoud Hassanein, MD, Alexandria University, Alexandria, Egypt, presented potential mechanisms by which increased sympathetic activity may result in effect blood pressure. As mentioned above, recent research has implicated the SNS in the development of hypertension, as sympathetic nervous activity can initiate and sustain blood pressure elevation. Although sympathetic denervation in the thoracic, abdominal, and pelvic regions has been demonstrated to decrease blood pressure in patients with malignant hypertension, they are associated with high morbidity, such as bowel, bladder, and erectile dysfunction; severe postural hypotension, and death.
Renal denervation has emerged as a treatment of resistant hypertension due to the observation that efferent sympathetic activity to the kidneys is higher in patients with hypertension [Esler M et al. Am J Hypertens 1989]. In addition, patients with hypertension demonstrate renal norepinephrine spillover, in which norepinephrine escapes neuronal uptake and local deactivation, allowing it to “spillover” into systemic circulation. Importantly, the efferent and afferent sympathetic nerves, which are located adjacent to the renal artery, are essential for systemic hypertension [DiBona GF. Curr Opin Nephrol Hypertens 2002]. An increase in renal sympathetic activity results in decreased sodium excretion, increased water retention, stimulation of the juxtaglomerular apparatus resulting in greater release of the enzyme renin, and changes to the renal blood flow. All of these characteristics contribute to both acute and long-term increases in blood pressure.
Dr. Hassanein highlighted a multicenter, proof-of-principle study, in which 45 patients with resistant hypertension with a mean of 4.7 antihypertensive medications were treated with percutaneous radiofrequency catheter-based therapy and followed for 1 year [Krum H et al. Lancet 2009]. The mean change in office blood pressure from baseline after the procedure is shown in Figure 2.

Effect of Renal Denervation on Office Blood Pressure
Reproduced from Krum H et al. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet 2009;373(9671):1275–1281. With permission from Elsevier.
Dr. Hassanein concluded that selective renal sympathetic denervation is a promising approach for the treatment of resistant hypertension, since it interrupts renal sympathetic activity without affecting nerves in the abdominal, pelvic, or lower extremity regions of the body. Ongoing clinical outcomes trials of renal denervation will determine whether it will become a standard treatment option for patients with resistant hypertension.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.