

Summary
Most hypertension guidelines are based on randomized studies that enrolled few black patients. In the Caribbean, treatment of hypertension is important especially in black patients, who suffer from higher rates of hypertension-associated morbidity and mortality (eg, diastolic dysfunction, heart failure, renal disease) than non-black patients. This article discusses successful pilot studies of a primarily black patient population using a database developed over a decade.
- Hypertensive Disease
- Cardiometabolic Disorder
- Cardiometabolic Disorder Clinical Trials
- Hypertensive Disease
- Cardiology & Cardiovascular Medicine
- Cardiometabolic Disorder
- Cardiology Clinical Trials
Most hypertension guidelines are based on randomized studies that enrolled few black patients. In the Caribbean, treatment of hypertension is important especially in black patients, who suffer from higher rates of hypertension-associated morbidity and mortality (eg, diastolic dysfunction, heart failure, renal disease) than non-black patients. Jobst Winter, MD, Thoracic Center Curacao, Willemstad, Netherlands Antilles, said that the cardiometabolic epidemic is only expected to worsen these impacts of hypertension in Afro-Caribbean populations. Dr. Winter described successful pilot studies conducted in the Thoracic Center's primarily black patient population using a database developed over a decade. They found evidence that even minimal reduction in blood pressure may result in measurable benefits including reductions in left ventricular hypertrophy (LVH) and increased exercise capacity.
Dr. Winter emphasized that most studies and guidelines are based on isolated clinic blood pressure (BP) measurements. Nighttime elevations and lack of diurnal BP variation also increase the risk for stroke and mortality. Studies were conducted to evaluate the effects of BP treatment in patients presenting with de novo hypertension without coronary artery disease; both studies used 24-hour BP measurements.
Study 1 included 234 hypertensive patients with a mean age of 55.5 years of whom 46% were male. Serial measurements of LV wall thickness were made during treatment of hypertension for mean follow-up of 550 days. LVH was determined by echocardiographic measurements of the intraventricular septum and left ventricular posterior wall. Follow-up studies will use ventricular mass as a more accurate measure of LVH.
Study 2 included 63 hypertensive patients with a mean age of 50.7 years, 57% of whom were male. Exercise capacity was measured using a treadmill exercise test. Maximal exercise was recorded in metabolic equivalents before treatment and after treatment. The mean follow-up was 236 days.
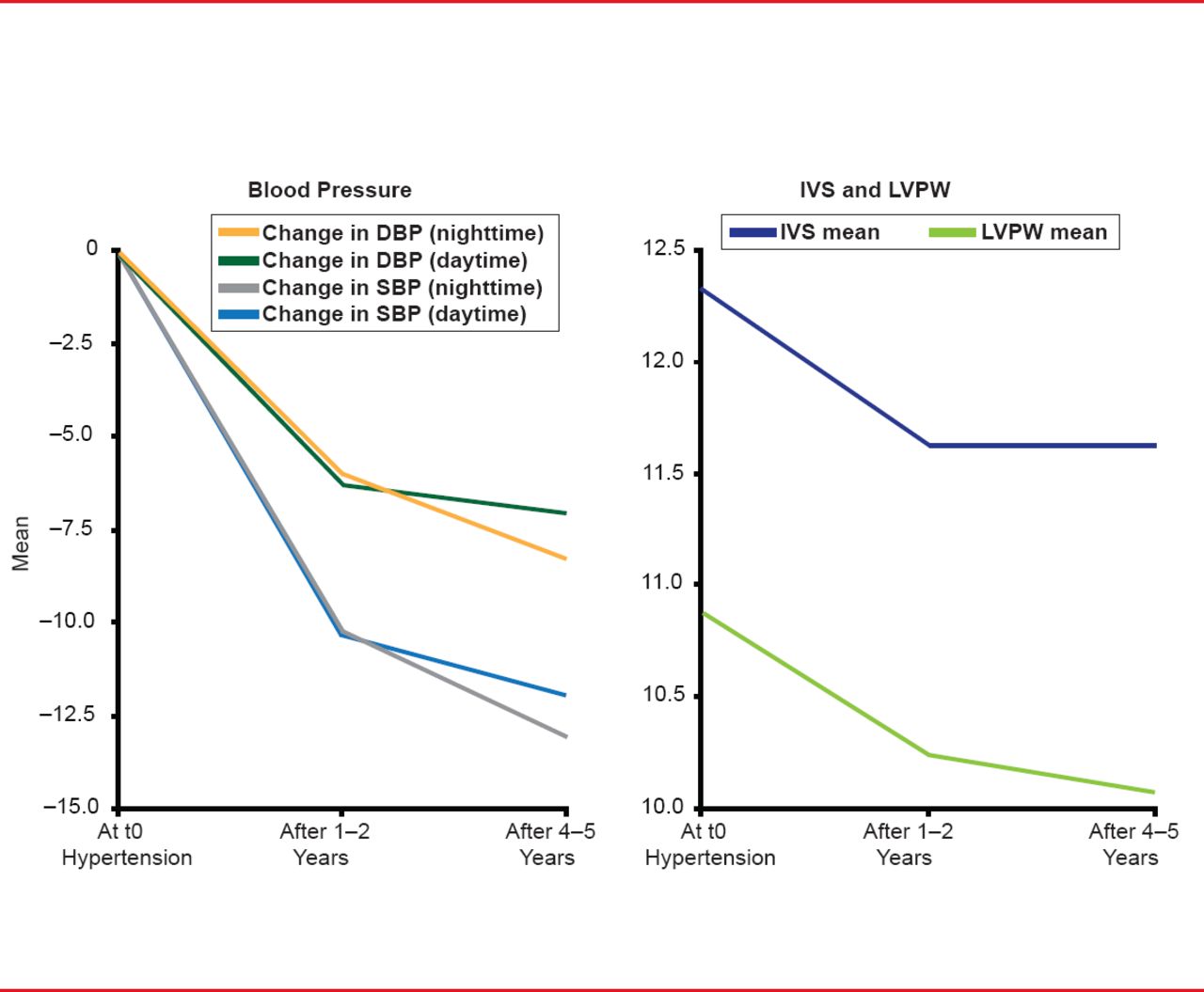
In Study 1, despite being titrated to an average of 3.2 antihypertensive agents, only small BP reductions were achieved. Although BP was lowered modestly, this cohort did not achieve guideline-based BP goals. The effect of BP on LVH was evaluated using mixed linear models adjusted for age, gender, and diabetes. The outcome, LVH, decreased during follow-up in association with reduction in blood pressure (Figure 1).

Change in BP and LV Wall Thickness During Follow-Up
DBP=diastolic blood pressure; IVS=intraventricular septum; LVPW=left ventricular posterior wall; SPB=systolic blood pressure.
Reproduced with permission from J Winter, MD.
In Study 2, despite being titrated to an average of 3.4 antihypertensive agents, only modest BP reductions were achieved similar to the findings in Study 1. This cohort also did not achieve guideline-based BP goals. The reductions in daytime and nighttime BP although modest, however, were correlated with an increased exercise capacity. These studies demonstrate potential benefits of BP lowering even if modest. In addition, they underscore the challenge in achieving guideline targets for BP control in this apparently treatment-resistant Afro-Caribbean population.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.