

Summary
The first percutaneous coronary intervention (PCI) was performed in the mid-1970s; however, PCI has been available in Guyana only since 2006. The Caribbean Heart Institute (CHI), a 5-bed inpatient facility with 1 catheterization lab, 1 resident cardiologist, 2 internists, and 12 nurses, was the first center in Guyana to perform PCI. This article presents results of a case series that assessed the clinical outcomes of all cases in whom percutaneous transluminal coronary angioplasty or stenting was attempted between January 1, 2011, and June 30, 2013.
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
- Interventional Techniques & Devices
The first percutaneous coronary intervention (PCI) was performed in the mid-1970s; however, PCI has been available in Guyana only since 2006. The Caribbean Heart Institute (CHI), a 5-bed inpatient facility with 1 catheterization lab, 1 resident cardiologist, 2 internists, and 12 nurses, was the first center in Guyana to perform PCI. CHI receives referrals from a 215,000-km2 area, which can potentially increase the time from symptom onset to revascularization.
Joel Joseph, MD, CHI, Georgetown, Guyana, presented results of a case series that assessed the clinical outcomes of all cases in whom percutaneous transluminal coronary angioplasty (PTCA) or stenting was attempted between January 1, 2011, and June 30, 2013. The outcomes assessed included death (at hospitalization, and at 30 days and 6 months post revascularization), acute renal failure, arrhythmias, myocardial infarction (MI), blood transfusions, and access site hematomas. Vital status of cases treated with PCI was confirmed either by medical record review or by phone. Death was confirmed by entry into the National Death Registry and cause of death on the death certificate.
Fifty-eight cases (mean age 58 ± 8 years; men—women ratio, 3:1) received revascularization. The success rate of revascularization (defined as TIMI 3 flow + < 25% stenosis post procedure) was 97%. Most cases (61%) had their intervention within 1 day of presentation; 86% were discharged within 2 days of intervention.
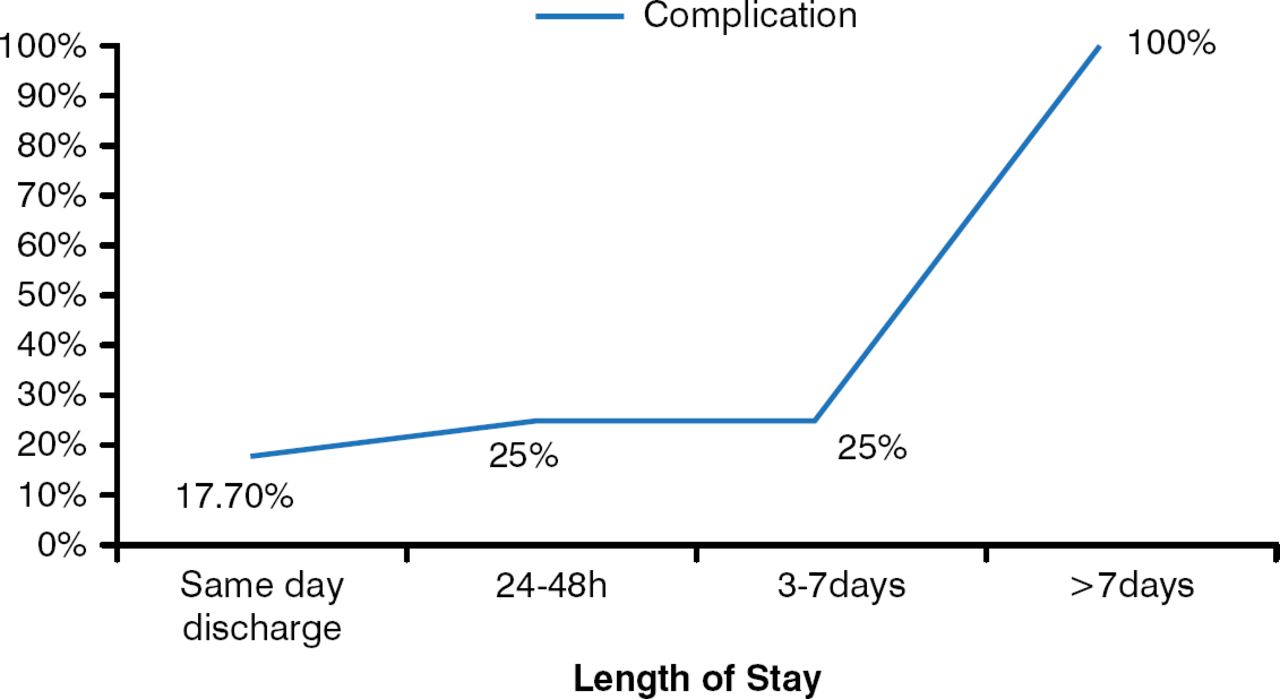
One case died after discharge from the hospital. She was a 56-year-old woman with diabetes, hypertension, and congestive heart failure as well as a history of prior PCI (2 years prior). The case was discharged within a day of her intervention, with no documented complications, and she was given a prescription for antiplatelet medication. She died 16 days later after failing to comply with dual-antiplatelet therapy and developing acute stent thrombosis. Of the 58 cases treated, 10 had an arrhythmia, 6 had an MI, and 3 had an access site hematoma. Acute renal failure and blood transfusion were reported in 1 patient each (1.72%). All cases remaining in hospital for more than 7 days had complications (Figure 1).

Complication Incidence Increased With Length of Hospital Stay
Reproduced with permission from J Joseph, MD.
Periprocedural complications were numerically greater, albeit not statistically significant, in men, cases aged > 55 years at the time of intervention, and those undergoing PCI for a ST-segment elevation myocardial infarction. Similarly, cases with > 28 days between symptom onset and intervention and those requiring multivessel revascularization had more periprocedural complications, but these were also not significant.
This study was limited in that it was a single-center observational study with no controls. There were few events, and it was difficult to confirm information from the records. Despite this, Dr. Joseph concluded that the success rates and outcomes of PCIs done at CHI were acceptable, especially considering the low volume of cases and the recent initiation of the PCI program.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.