

Summary
In her inaugural speech at her swearing in as the 64th president of the American Congress of Obstetrics and Gynecology (ACOG) at the 2013 annual meeting, Jeanne A. Conry, MD, PhD, used the mantra “Every Woman, Every Time” to highlight the importance of addressing reproductive health in women at every opportunity. This article discusses the advantages of long-acting reversible contraceptives, best emergency contraception, transcervical sterilization, as well as evidence-based guidelines for contraceptive use.
- Pregnancy
- Obstetrics & Gynecology
- Pregnancy
In her inaugural speech at her swearing in as the 64th president of the American Congress of Obstetrics and Gynecology (ACOG) at the 2013 annual meeting, Jeanne A. Conry MD, PhD, used the mantra “Every Woman, Every Time” to highlight the importance of addressing reproductive health in women at every opportunity.
During a session at the 2014 ACOG annual meeting that updated participants on issues they need to know about contraceptives in 2014, Eve Espey MD, MPH, and Tony Ogburn, MD, Department of Obstetrics and Gynecology, University of New Mexico, Albuquerque, New Mexico, USA, echoed this message emphasizing the need for gynecologists to consider every visit by a woman of reproductive age an opportunity to discuss contraception.
Prof. Espey urged participants to treat any woman who is interested in a contraceptive as an emergency and to schedule her in for a visit as soon as possible. She also emphasized the need to remove barriers such as the 2-visit requirements for insertion of intrauterine devices (IUDs) and implants.
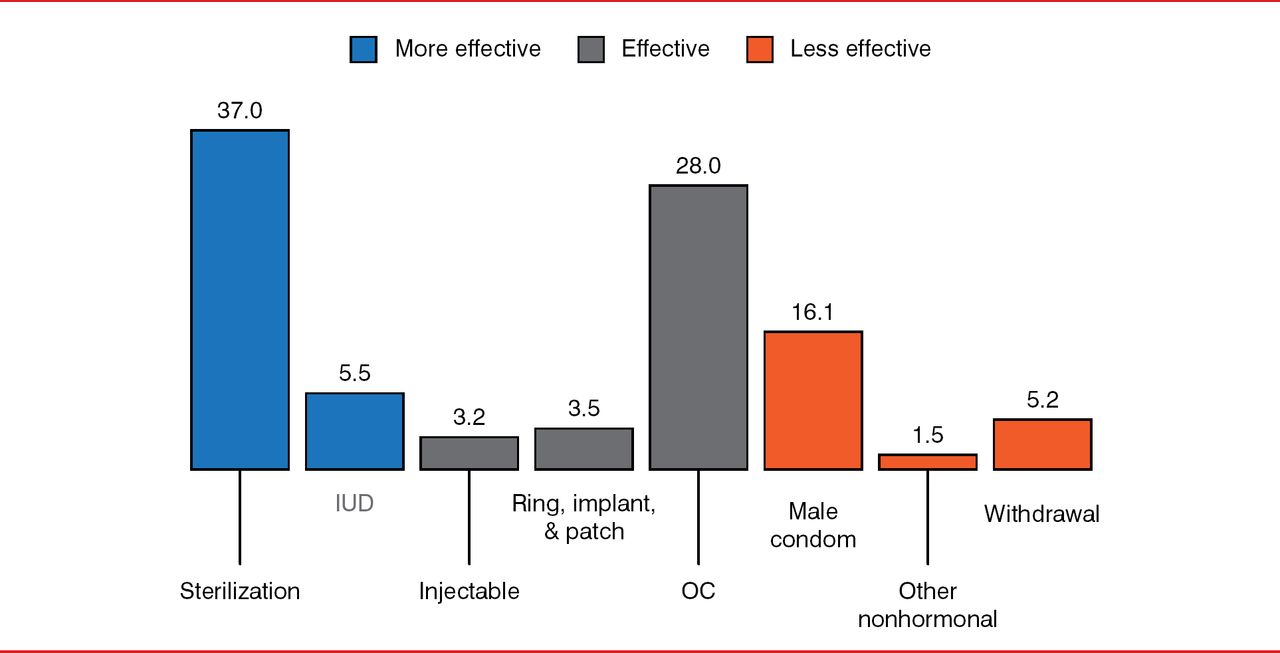
She also highlighted the need to help women decide on using more effective methods of contraception, saying that women using contraceptives in the United States make up 89% of the women at risk of unintended pregnancies and 53% of women with unintended pregnancies. Figure 1 shows the types of contraceptives used in the United States.

US Contraceptive Use (2006 to 2008; percentage)
IUD=intrauterine devices; OC=oral contraceptive.
Source: Vital Health Stat. Aug 2010;23(29):1–44.
Among the topics discussed during the session were the advantages of long-acting reversible contraceptives (LARCs), current guidelines on contraceptives, and the advantages and limitations of transcervical sterilization.
ADVANTAGES OF LONG-ACTING REVERSIBLE CONTRACEPTIVES
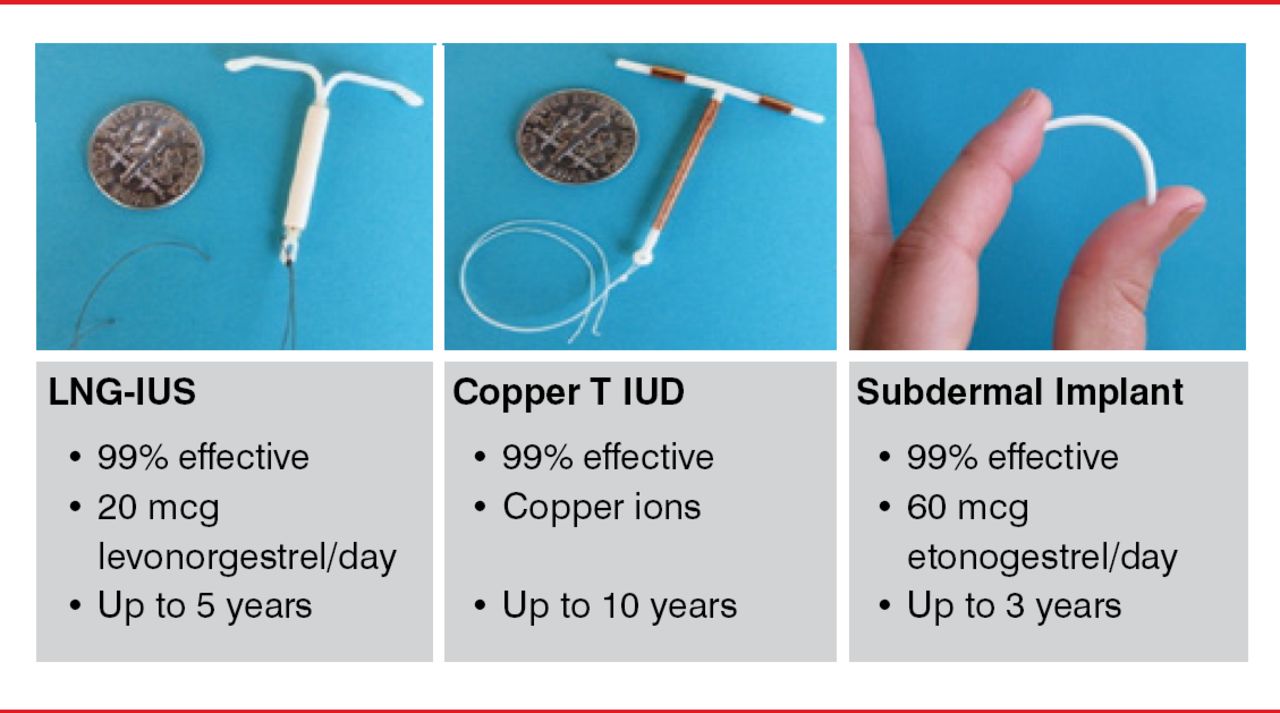
Prof. Espey walked participants through the current evidence showing the advantages of (LARCs) over short-acting contraceptives to prevent pregnancies, both in adolescents and in nulliparous women. Three types of LARCs are currently available, all of which show a 99% efficacy (Figure 2).

Types of Long-Acting Reversible Contraceptives
Reproduced with permission from Eve Espey, MD, MPH.
Citing the Contraceptive Choice Project study [CHOICE; Peipert JF et al. Obstet Gynecol 2012], in which almost 10,000 women desiring contraception were given their choice of all methods at no cost along with counseling, she said the study showed that most women (76%) chose an LARC and that 80% were satisfied with an IUD compared with 54% who were satisfied with the pill, patch, or ring.
The superior efficacy of a LARC was shown by the study finding that the risk of failure was 20 times higher in women who chose pills, the patch, or the ring compared to those who chose a LARC. The study also showed that women in the CHOICE study had a significant reduction in abortion rates compared to the general population (6 per 1000 vs 20 per 1000, respectively; p<0.001), representing a prevention of 1 abortion for every 108 women given free contraception. In addition, the CHOICE study found a reduction in teenage births compared with the general population (6 per 1000 vs. 34 per 1000, respectively).
Prof. Espey said that data coming from the CHOICE study will continue to provide a treasure trove for years to come.
BEST EMERGENCY CONTRACEPTION
By far the most effective method for emergency contraception is the copper IUD, said Prof. Espey, which can be placed up to 7 days after unprotected intercourse. Also recommended is 30 mg ulipristal acetate, which she believes is a well-kept secret that gynecologists need to know about. The first selective progesterone receptor modulator approved by the Food and Drug Administration, the sole mechanism of action is to delay ovulation and is effective in preventing pregnancy up to 5 days after having unprotected sex. She cited data showing the superior efficacy of 30 mg ulipristal acetate compared with 1.5 mg levonorgestrel (odds ratio of 0.55 if used within 120 hours and 0.35 if used within 24 hours) [Glasier AF et al. Lancet 2010].
She emphasized that ulipristal acetate is available only by prescription and said that it is the only emergency contraception that she writes a prescription for. She encouraged gynecologists to do the same if they are involved in prescribing an emergency contraception, saying that ulipristal acetate also has very few side effects.
TRANSCERVICAL STERILIZATION
Prof. Ogburn discussed the advantages and limitations of transcervical sterilization, emphasizing that it is a good procedure and, particularly for specific women such those who are obese, is a recommended procedure. Advantages include no anesthesia or incisions needed, ability to perform as an outpatient procedure, less pain and shorter recovery, and potentially being less expensive. Limitations, he said, include the lack of immediate efficacy and the need to use an alternative contraceptive until hysterosalpinography is performed 3 months after the procedure to ensure blockage of tubes, the need for specialized equipment and training, and the lack of data on long-term effects.
He cautioned, however, that patients should be told of the varying success rates reported on first attempt at the bilateral placement of the coils. He cited real-life clinical data from the experience at his institution between 2005 and 2012 that showed a success rate of only 89.5%, which translates into about 1 out of 10 occurrence of not successfully placing the coils at first attempt. Based on these data, he said that he and his colleagues have changed their practice and now include this information when counseling patients about this option. They also inform patients that about 3% will not have complete occlusion on hysterosalpinography at 3 months among those in whom bilateral placement is achieved.
EVIDENCE-BASED GUIDELINES FOR CONTRACEPTIVE USE: UNITED STATES MEDICAL ELIGIBILITY CRITERIA
Prof. Espey recommended that participants refer to the 2013 “United States Medical Eligibility Criteria (USMEC) for Contraceptive Use” to help counsel individual patients on contraceptive use based on different patient and disease characteristics [CDC 2014]. Developed by the Centers for Disease Control and Prevention, the evidence-based guidelines are free, downloadable charts that can be displayed in the office and be downloaded as an app for easy referral, as she does. The charts provide easy-to-read recommendations based on 4 categories and are color coded either as green (use recommended) or red (use not recommended).
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.