

Summary
Aortic complications are an important cause of death in patients with giant-cell arteritis (GCA). Extracranial involvement of large vessels in patients with GCA probably is underdiagnosed. 18-fluoro-deoxyglucose (FDG) positron emission tomography (PET) offers good sensitivity for the detection of large vessel involvement in patients with GCA [Blockmans D et al. Arthritis Rheum 2006; Besson FL et al. Eur J Nucl Med Mol Imaging 2011]. The objectives of this study were to characterize large vessel involvement using PET in a cohort of patients with GCA, describe the patients who had aortic complications, and identify factors associated with aortic complications.
- Tomography
- Imaging Modalities
- Vasculitis
- Inflammatory Disease Clinical Trials
- Inflammatory Disorders
- Tomography
- Rheumatology
- Imaging Modalities
- Vasculitis
- Inflammatory Disease
- Rheumatology Clinical Trials
- Inflammatory Disorders
Aortic complications are an important cause of death in patients with giant-cell arteritis (GCA). According to Hubert de Boysson, MD, Centre Hospitalier et Universitaire Cote de Nacre, Caen, France, extracranial involvement of large vessels in patients with GCA probably is underdiagnosed.
18-fluoro-deoxyglucose (FDG) positron emission tomography (PET) offers good sensitivity for the detection of large vessel involvement in patients with GCA [Blockmans D et al. Arthritis Rheum 2006; Besson FL et al. Eur J Nucl Med Mol Imaging 2011]. The objectives of this study were to characterize large vessel involvement using PET in a cohort of patients with GCA, describe the patients who had aortic complications, and identify factors associated with aortic complications.
Patients included in this retrospective observational study met at least three American College of Rheumatology (ACR) criteria for GCA (or two criteria plus extra-temporal biopsy-proven giant-cell vasculitis), had at least one PET at diagnosis or during follow-up, and had an aortic morphology assessment at diagnosis and during follow-up. Patients with aortic complications at diagnosis were excluded. A positive PET was defined as FDG vascular uptake superior to the liver in at least one of the following vascular segments: thoracic or abdominal aorta, or subclavian, axillary, carotid, upper limb, ilio-femoral, or lower limb arteries.
In total, 129 patients met the criteria and were followed for 35 months. Baseline characteristics, clinical characteristics and cardiovascular risk factors were similar in the entire cohort between patients with aortic complications and those without complication. Among the 129 patients, 65 (50%) had PET at diagnosis (ie, before or in the 10 first days of the treatment) and 64 (50%) had PET during follow-up. Aortic complications occurred in a total of 10 patients: 6 patients (60%) who had PET at diagnosis and 4 patients (40%) who had PET during follow-up.
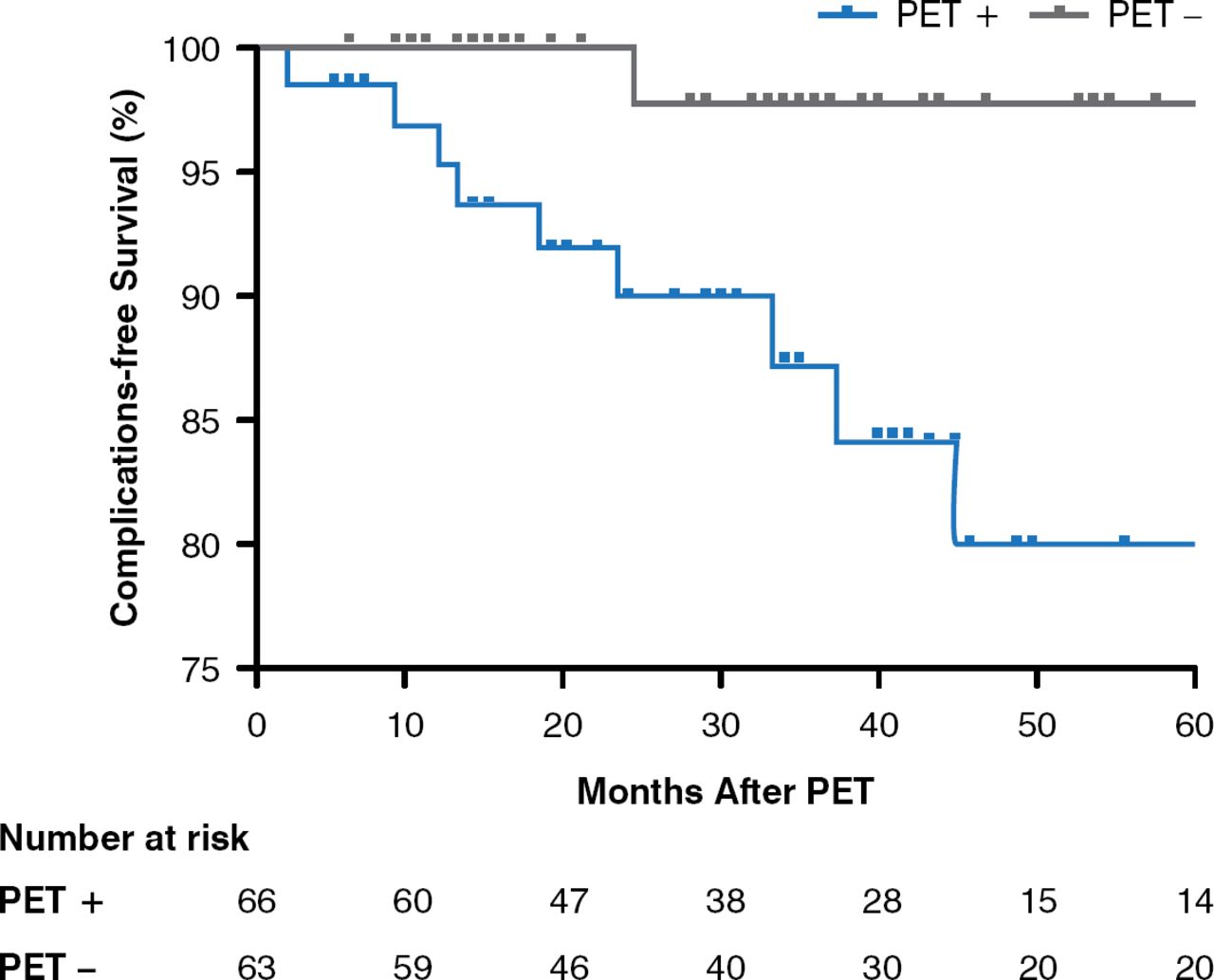
Sixty-four (50%) patients had a positive PET (55% at diagnosis, 44% during follow-up). The three most-involved vascular areas were thoracic aorta (81%), subclavian arteries (73%), and abdominal aorta (58%). Nine of the 10 patients with aortic complications had a positive PET compared with 55 of 119 patients without complications (90% vs. 46%, p=0,008). Complications occurred at a median time of 19.5 (range, 3 to 43) months after PET and 27.5 (3 to 180) months after diagnosis. In the univariable analysis, patients with a positive PET had a significantly higher risk of developing aortic complications as compared with those with a negative PET (HR, 9.2; 95% CI, 1.2 to 72.7; p=0.01; Figure 1).

Risk of Aortic Complications in Patients With a Positive Versus Negative PET
PET=positron emission tomography.
Reproduced with permission from H de Boysson, MD.
Among the 10 patients with aortic complications, the thoracic section was of a concern for 9 patients (8 had thoracic aorta dilatation or aneurysm, and 1 had aortic dissection), whereas 1 patient had an abdominal aorta aneurysm. Patients with a positive PET versus those with a negative PET had more extra-cephalic manifestations (64% vs 37%; p=0.002) and fewer cephalic symptoms (72% vs 89%; p=0.01). There were 7 deaths, including 2 from strokes, 2 from myocardial infarctions, 1 from colitis, 1 from pneumonia, and 1 from limb ischemia. Three of 5 patients with a cardiovascular event had a positive PET.
This study suggested that patients with GCA who had a positive PET at diagnosis or during follow-up had a higher risk of developing aortic complications. These patients had an atypical presentation with more extra-cephalic symptoms and fewer cephalic manifestations than is typically observed in GCA. Prospective studies are needed to confirm these results.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.