

Summary
Thrombosis of the dural venous sinus and/or cerebral veins (CVT) is a very complex problem that remains somewhat poorly understood. Yet, although it is an important consideration in cases of stroke, the evidence base for its medical and interventional management is lacking. This article discusses current perspectives on the pathogenesis and risk factors for CVT development, as well as treatment options. Other topics include the epidemiology and risk factors for CVT, medical management of CVT, as well as appropriate use of acute endovascular intervention.
- Thrombotic Disorders
- Cerebrovascular Disease
- Ischemia
- Interventional Techniques & Devices
- Thrombotic Disorders
- Cerebrovascular Disease
- Ischemia
- Interventional Techniques & Devices
- Neurology
Thrombosis of the dural venous sinus and/or cerebral veins (CVT) is a very complex problem that remains somewhat poorly understood. Yet, although it is an important consideration in cases of stroke, the evidence base for its medical and interventional management is lacking. Fernando Barinagarrementeria, MD, St. Universidad del valle de Mexico de Querétaro, Mexico, launched a series of sessions that covered current perspectives on the pathogenesis and risk factors for CVT development, as well as treatment options. Data were presented from some of the clinical trials in medical management and acute endovascular intervention in these patients in an effort to guide physicians in decision-making when evidence is lacking.
PATHOGENESIS
The risk factors for CVT are linked to Virchow's triad of factors that comprises the three broad categories of components that contribute to thrombosis: hypercoagulability, blood stasis, and endothelial damage [Saposnik G et al. Stroke 2011].
Although the exact mechanism of clot formation in the central venous system is not well understood, thrombosis here results in outflow obstruction, venous congestion, and increased hydrostatic pressure, which drive fluid into the interstitium and cause edema. Sustained increase in intracerebral pressure may subsequently lead to parenchymal abnormalities in the form of venous infarction or intracerebral hemorrhage (ICH) [Dlamini N et al. Neurosurg Clin N Am 2010].
EPIDEMIOLOGY AND RISK FACTORS FOR CEREBRAL VEIN THROMBOSIS
CVT is considered an uncommon form of a stroke, comprising 0.5% to 1.0% of all cases. It is, however, becoming an increasingly recognized cause. Numerous risk factors are involved in its development, and include young age, being female, pregnancy/puerperium, oral contraceptive use, and thrombophilia [Saposnik G et al. Stroke 2011]. Risk factors for an unfavorable clinical outcome include being male, age >37 years, mental status disorder, coma, ICH on admission, thrombosis of the deep cerebral venous system, central nervous system infection, and malignancy (Table 1) [Li G. Neurosurg 2013; Ferro JM et al. Stroke 2004].
Risk Factors for an Unfavorable Outcome in Patients With CVST
MEDICAL MANAGEMENT OF CEREBRAL VEIN THROMBOSIS
Options for treatment of CVT are limited, and there is a paucity of evidence-based regimens for medical management of these patients. Although thrombolytic agents are used in ischemic stroke, they are not a consideration in patients with CVT due to the potential for hemorrhage. Steroid use is also contraindicated [Saposnik G et al. Stroke 2011].
Gene Y. Sung, MD, MPH, Keck School of Medicine, University of Southern California, Los Angeles, California, USA, discussed some of the data that are available in this patient population. He highlighted that while anticoagulant treatment of CVT has been controversial due to the associated risk of ICH, data from trials continue to demonstrate its effectiveness in this setting, and it remains the mainstay of medical management for patients.
In 1991, data were reported from a small randomized, placebo-controlled trial that evaluated anticoagulation with adjusted-dose intravenous heparin for treatment of aseptic CVT in 20 patients [Einhäupl KM et al. Lancet]. The primary endpoint was CVT severity score and treatment was randomized to nothing or 3000 units of a heparin bolus, and then a partial thromboplastin time goal of 2x baseline. A difference in clinical course was evident in favor of the heparin group after only 3 days of treatment (p<0.05) and this remained significant (p<0.01) after 8 days of treatment. After 3 months, in the heparin-treated group (n=10), 8 patients had a complete clinical recovery and 2 had minor neurological deficits; there was no mortality, and no new ICHs developed (3/10 had prior ICH at baseline). In the placebo group (n=10), only 1 patient had a complete recovery, 6 patients had neurological deficits; 3 patients died (p<0.01), and 2 new ICHs developed in this group. Although this study involved only a small number of participants, the mortality rate of 30% versus 0% in placebo and treatment groups was a statistically significant finding (p<0.05) in favor of anticoagulant treatment, and led to early cessation of the trial.
Later, a 2002 Cochrane Review reported a meta-analysis of available evidence regarding the effectiveness and safety of anticoagulant therapy in patients with CVT [Stam J et al. Cochrane Database Syst Rev 2002]. It evaluated data from 2 small, randomized controlled trials (RCTs) that compared anticoagulant therapy with placebo or open control in CVT. Data demonstrated that anticoagulant therapy was associated with a pooled relative risk of death of 0.33 (95% CI, 0.08 to 1.21), and of death or dependency of 0.46 (95% CI, 0.16 to 1.31). No new ICHs developed, although major gastrointestinal hemorrhage occurred after anticoagulant treatment in 1 patient and in 2 patients in the placebo arm experienced probable pulmonary embolism, one of which was fatal. Although the results were not statistically significant, they showed a trend toward benefit in the form of a potentially important reduction in the risk of death or dependency. Based on the limited evidence available, it was concluded that anticoagulant treatment for CVT seems to be safe.
In 2006, the American Heart Association/American Stroke Association Scientific Statement provided recommendation for managing patients with CVT [Sacco RL et al. Stroke 2006]. They concluded that low-molecular-weight heparin (LMWH) is a reasonable treatment option, even in the presence of hemorrhagic infarction, and that continuation of oral anticoagulant therapy for 3 to 6 months, followed by antiplatelet therapy, was reasonable.
ACUTE ENDOVASCULAR INTERVENTION IN PATIENTS WITH CEREBRAL VEIN THROMBOSIS
Despite aggressive anticoagulant therapy, however, 9% to 13% of patients with CVT still have a very poor outcome, noted Charles I. Prestigiacomo, MD, Neurological Institute of New Jersey, Newark, New Jersey, USA. Although evidence for use of endovascular management of CVT is also lacking, he added that some observational studies demonstrate that if deterioration persists despite maximum anticoagulant management, endovascular therapy (ET) maybe warranted as a final salvage effort.
WHEN IS ENDOVASCULAR THERAPY INDICATED?
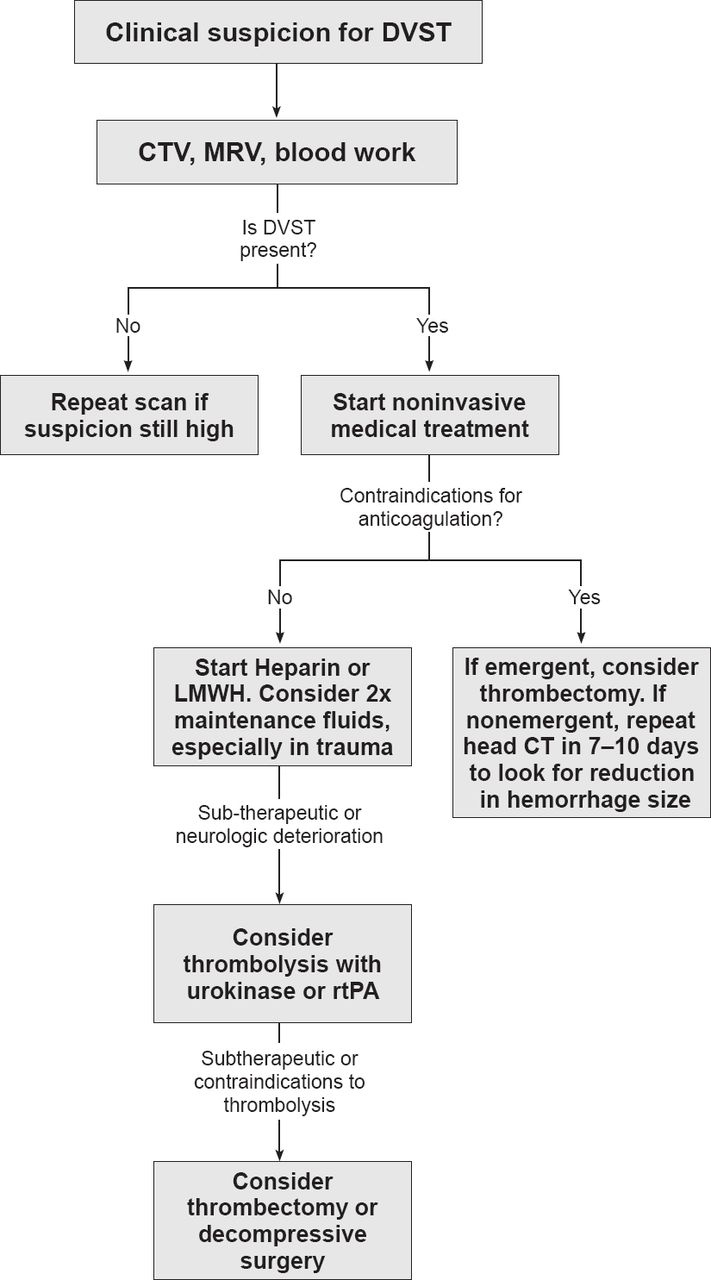
Although it is clear that increasing venous outflow improves patient outcomes, it remains difficult to know when to choose this technique. However, recent publication of a proposed treatment algorithm has provided some guidance for physicians where little evidence exists (Figure 1) [Gala NB et al. J Neurointerven Surg 2013]. The algorithm highlights the need to initially identify the underlying cause of the CVT. It also indicates intravenous heparin or LMWH as first-line treatment. Thrombolytic treatment should only be instituted if the patient fails to improve or has risk factors, such as coma, for a poor prognosis. And only if there are serious findings on imaging studies, or if the patient is severely disabled, should emergent ET be considered. Rheolytic thrombectomy followed by thrombolysis to dissolve residual thrombi seems to produce good patient outcomes with appropriate long-term physical rehabilitation.

Treatment Algorithm for Patients With CVT
DVST=dural venous sinus thrombosis; CTV=computed tomography venography; MRV=magnetic resonance venography; LMWH=low molecular weight heparin; CT= computed tomography; rt-PA= recombinant tissue plasminogen activator.
Reproduced from Gala NB et al. Current endovascular treatment options of dural venous sinus thrombosis: a review of the literature. J Neurointerven Surg 2013;;5(1):28–34. With permission from the BMJ Publishing Group.
The Thrombolysis Or Anticoagulation for Cerebral Cenous Thrombosis trial [TO-ACT; NCT01204333; Coutinho JM et al. Int J Stroke 2013] is a multicenter, prospective, open-label, randomized study that is currently recruiting participants. It will aim to determine if ET improves the functional outcome of patients with a severe form of CVT. The primary endpoint of this study is the mRS score at 12 months. Dr Prestigiacomo hopes that emerging data from this trial will provide more insight into outcomes in CVT. He concluded that additional RCTs will be essential to provide evidence for best practices in how to medically and interventionally manage patients with this condition.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.