

Summary
The American Heart Association (AHA)/American Stroke Association (ASA) guidelines recommend a door-to-needle (DTN) time of =60 minutes for reperfusion therapy for acute ischemic stroke patients [Jauch EC et al. Stroke 2013]. The rapid treatment is important for improving stroke outcome, but many studies have concluded that this time frame has been met by <30% of intravenous tissue plasminogen activator (t-PA)-treated stroke patients. This article discusses the principal results from the Target: Stroke Initiative, a national program organized by the AHA/ASA, which addresses this timing dilemma by increasing the proportion of stroke patients with DTN time frames of <60 minutes.
- Cerebrovascular Disease
- Neurology Clinical Trials
- Cerebrovascular Disease
- Neurology Clinical Trials
- Neurology
The American Heart Association (AHA)/American Stroke Association (ASA) guidelines recommend a door-to-needle (DTN) time of ≤60 minutes for reperfusion therapy for acute ischemic stroke patients [Jauch EC et al. Stroke 2013]. The rapid treatment is important for improving stroke outcome, but many studies have concluded that this time frame has been met by <30% of intravenous tissue plasminogen activator (t-PA)-treated stroke patients.
Gregg C. Fonarow, MD, University of California Los Angeles, Los Angeles, California, USA, presented the principal results from the Target: Stroke Initiative, a national program organized by the AHA/ASA, which addresses this timing dilemma by increasing the proportion of stroke patients with DTN time frames of <60 minutes. The primary goal of the study was to treat at least 50% of acute ischemic stroke patients at Get With The Guidelines (GWTG)-Stroke participating hospitals and see that they were treated within 60 minutes of their arrival to the hospital [Fonarow GC et al. Stroke 2011]. In performing this assessment, 10 key evidence-based strategies were utilized to meet the goal (Table 1).
Evidence-Based Strategies to Reduce DTN Time
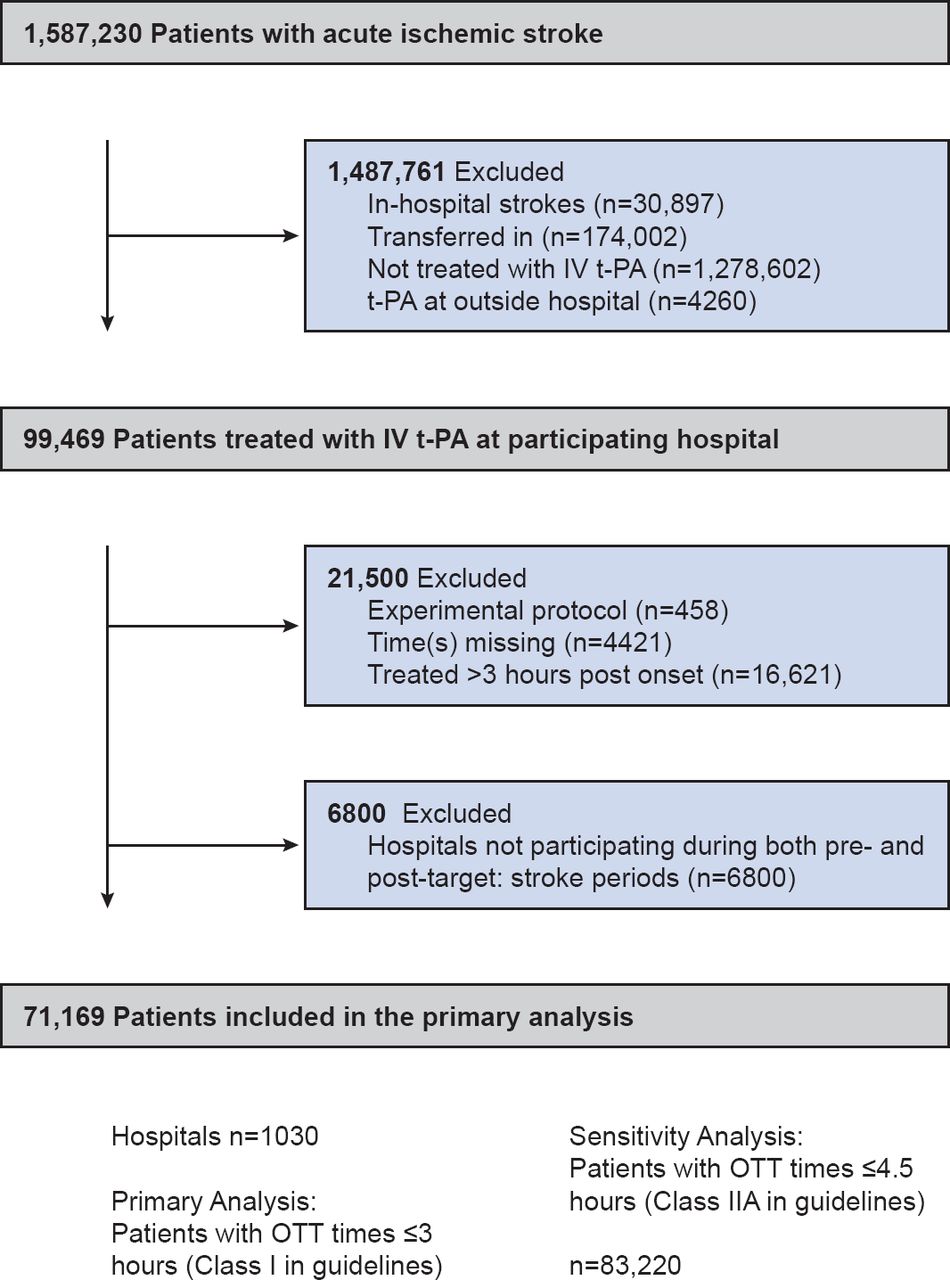
This study included various ongoing adjustments as they related to assessing the variables of patients and characteristics. Assessments were made of in-hospital mortality, discharge destination, ambulatory status, and symptomatic intracranial hemorrhage ≤36 hours following t-PA administration. Patient profiles included a balance of men and women, median age 72 years, who were of white, Hispanic, and black origins. Of the stroke patients treated with t-PA (n=71,169) 27,319 were pre-intervention and 43,850 were postintervention patients from 1030 GWTG-Stroke participating hospitals (Figure 1).

Selection of Study Population for Target: Stroke
IV=intravenous; OTT=onset to treatment; t-PA= tissue plasminogen activator.
Prior to the study's initiation in 2009, 15.6% of hospitals had DTN rates of ≤60 minutes in ≥50% of t-PA-treated stroke patients. Median time was 74 minutes in Quarter 4 of 2009, immediately prior to the start of the Target: Stroke initiative. The study's DTN goal was subsequently met by 46.7% of the participating hospitals by 2013 (p<0.0001) and by 53.3% of patients by Quarter 3, 2013 (p<0.0001). The program's goal of DTN times of ≤60 minutes was achieved within 4 years as opposed to the originally projected 15 years.
With a target of achieving a more rapid administration of t-PA, there were initial concerns centered on the shorter DTN times as related to rushed overall assessments for acute ischemic stroke patients. The Target: Stroke Initiative research revealed that rapid reperfusion therapy in acute ischemic stroke can be done with process reductions and improved outcomes.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.