

Summary
The marked, steady increase in the use of prescribed opioids since 2000 is matched by a steady increase in death by drug overdose. In 2008, death by drug overdose surpassed motor vehicle accidents as the leading cause of accidental death in the United States [Warner M et al. National Center for Health Statistics Data Brief #81. 2011]. This article discusses changes in prescription policy, as well as insights into current prescribing patterns, problematic opioid use, and education needs.
- Orthopaedic Pain Management
- Orthopaedic Pain Management
- Orthopaedics
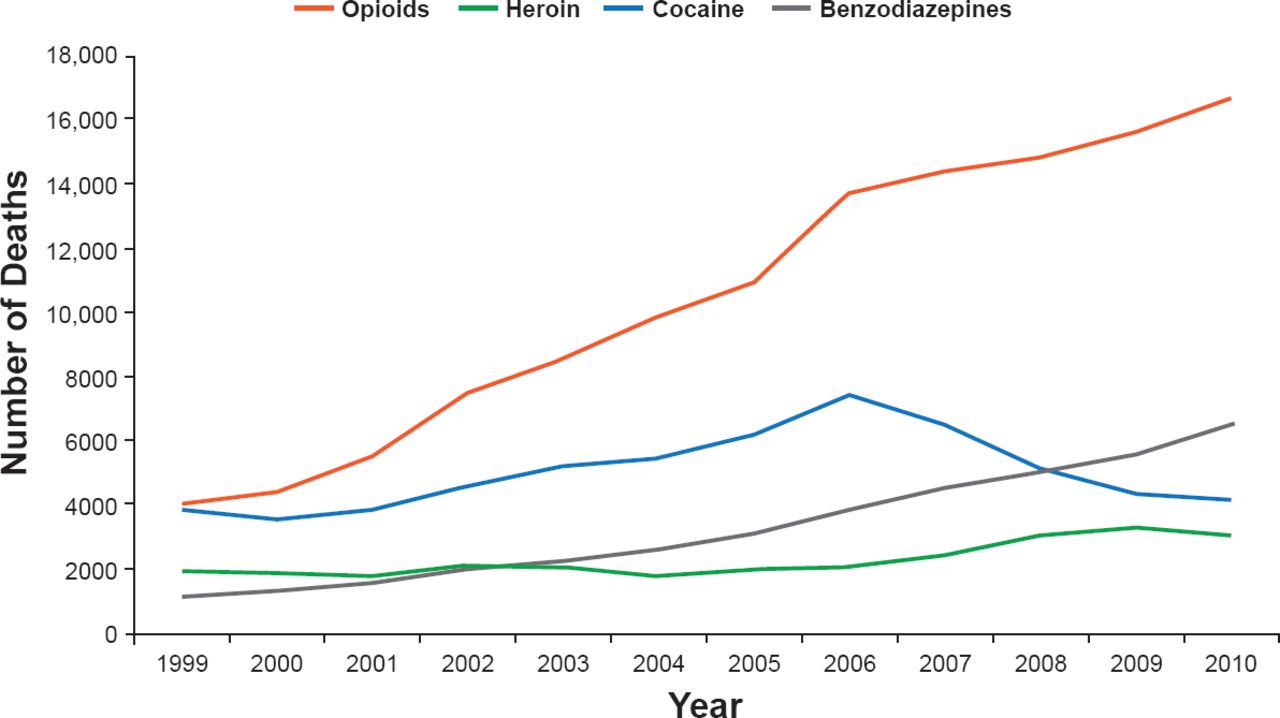
The marked, steady increase in the use of prescribed opioids since 2000 is matched by a steady increase in death by drug overdose (Figure 1). In 2008, death by drug overdose surpassed motor vehicle accidents as the leading cause of accidental death in the United States [Warner M et al. National Center for Health Statistics Data Brief #81.2011]. Andrew W. Gurman, MD, Altoona Hand and Wrist Surgery, Altoona, Pennsylvania, USA, stated this is not a street drug problem, with most of the available opioids prescribed by physicians.

Rates of Drug Overdose Deaths by Major Types of Drugs, USA, 1999–2010
Source: CDC, National Center for Health Statistics, National Vital Statistics System, CDC Wonder. Updated with 2010 mortality data.
Hydrocodone is the most widely prescribed (131.2 million) medication in the United States [IMS Institute for Healthcare Informatics. The Use of Medicines in the United States: Review of 2010. 2011]. However, 7 million people are opioid addicts and there are 12 million nonmedical users. Dr. Gurman stressed there is a 66% likelihood a patient will still be taking hydrocodone if they take it every day for 90 days, regardless of the reason for taking it [Martin BC et al. J. Gen Intern Med 2011 ONDCP. http://whitehousedrugpolicy.gov/publications/pdf/rx_abuse_plan.pdf].
Opioid diversion is the major source of nonmedically used prescription drugs. Nearly 56% are obtained from friends or relatives, 9% are purchased from friends or relatives, and 5.4% are taken from friends or family without their knowledge [Substance Abuse and Mental Health Services Administration. Results from the 2008 National Survey on Drug Use and Health: National Findings (Office of Applied Studies, NSDUH Series H-36, HHS Publication No. SMA 09-4434). Rockville, MD 2009].
One factor contributing to increased prescriptions of opioid analgesics is quality improvement efforts related to pain management. The Joint Commission requires a plan to assess pain, and there has been some movement by others to include pain measurement as the fifth vital sign. Also, reimbursement from the Centers for Medicare and Medicaid Services will be tied to patient satisfaction, which includes pain management. Further, said Dr. Gurman, time pressures for office visits and lack of reimbursement for treatment and evaluation of addiction are contributors, as well as physicians caring about suffering and having long-term relationships with their patients.
INSIGHTS FROM THE AAOS SURVEY OF FELLOWS
A survey conducted by the American Academy of Orthopaedic Surgeons (AAOS) provided insights into current prescribing patterns, problematic opioid use, and education needs. A total of 363 (12%) of 3000 AAOS Fellows responded to the Internet-based survey, 25% of whom were general surgeons, primarily performing surgery for hip fractures, long bone fractures, knee arthroplasty, anterior cruciate ligament, carpal tunnel, and trigger finger release, said David C. Ring, MD, Massachusetts General Hospital, Boston, Massachusetts, USA.
The stronger opioids, oxycodone and hydrocodone, were prescribed most frequently (range, 33%–63%) at discharge by these surgeons. Dr. Ring noted this was true even for carpal tunnel and trigger finger release surgery. The postoperative duration of opioid prescription ranged from 1 to 7 weeks. An established policy for opioid prescription use for the physician practice was reported by 68%. Dr. Ring noted this is the most effective way to control opioid prescriptions. Seventy-four percent said they would not refill an opioid prescription written by a partner. In 1% to 25% of cases, 86.2% said they would seek help from a pain specialist.
A prevalence of problematic opioid use in ≥5% of their practice patients was reported by 75% of surgeons. And 48% said that prescribing patterns of orthopedic surgeons contribute to misuse. Further, 58.7% said that tighter regulatory control for ease of access and prescription renewal is needed, while 33% were neutral and 8% said no.
The most important influence on their practice of opioid prescription was what they felt was effective (4.55 on a scale of 0 to 5) and what they were taught (2.51). Although 80% of surgeons said they could tell which patients would be a problem and they had the required communication skills to discuss appropriate opioid use with their patients, 29% said they needed help with communication strategies and setting limits. Guidelines for appropriate opioid prescribing for acute pain were requested by 72.5% of surgeons; for chronic pain by 55.6%; educational materials for limit setting and communication strategy by 80.4%; and for nonopioid pain management by 70%.
SINGLE-CENTER STUDY LED TO CHANGES IN PRESCRIPTION POLICY
A study by an orthopedic practice with five surgeons showed that 77% of the pills prescribed for pain after outpatient upper extremity surgery were not used, based on patient self-reporting [Rodgers J et al. J Hand Surg Am 2012]. Jeffrey Rodgers, MD, Des Moines Orthopaedic Surgeons, Des Moines, Iowa, USA, said their findings led to changes in prescribing patterns by their practice that have been effective.
A total of 250 patients were interviewed by phone between 7 and 14 days after surgery to confirm the medication and regimen prescribed and determine satisfaction with pain control, number of tablets remaining, and whether other analgesic medications were taken. The average of the patients was 54 years and 66.8% were women. Soft tissue surgery was performed in 76.7% and hard tissue in 23.3%.
All of the surgeons prescribed 30 pills, which Dr. Rodgers stated tends to be usual practice by all physicians, although there is no evidence to support this number or information regarding the tradition of this norm. Hydrocodone was prescribed for 51% of the patients, oxycodone for 24%, and propoxyphene for 23%. The pain score was reported to be between 0 and 2 by ∼68% of patients. The patients who had hard tissue surgery used more opioids compared with soft tissue surgery (14 vs 9 pills, respectively).
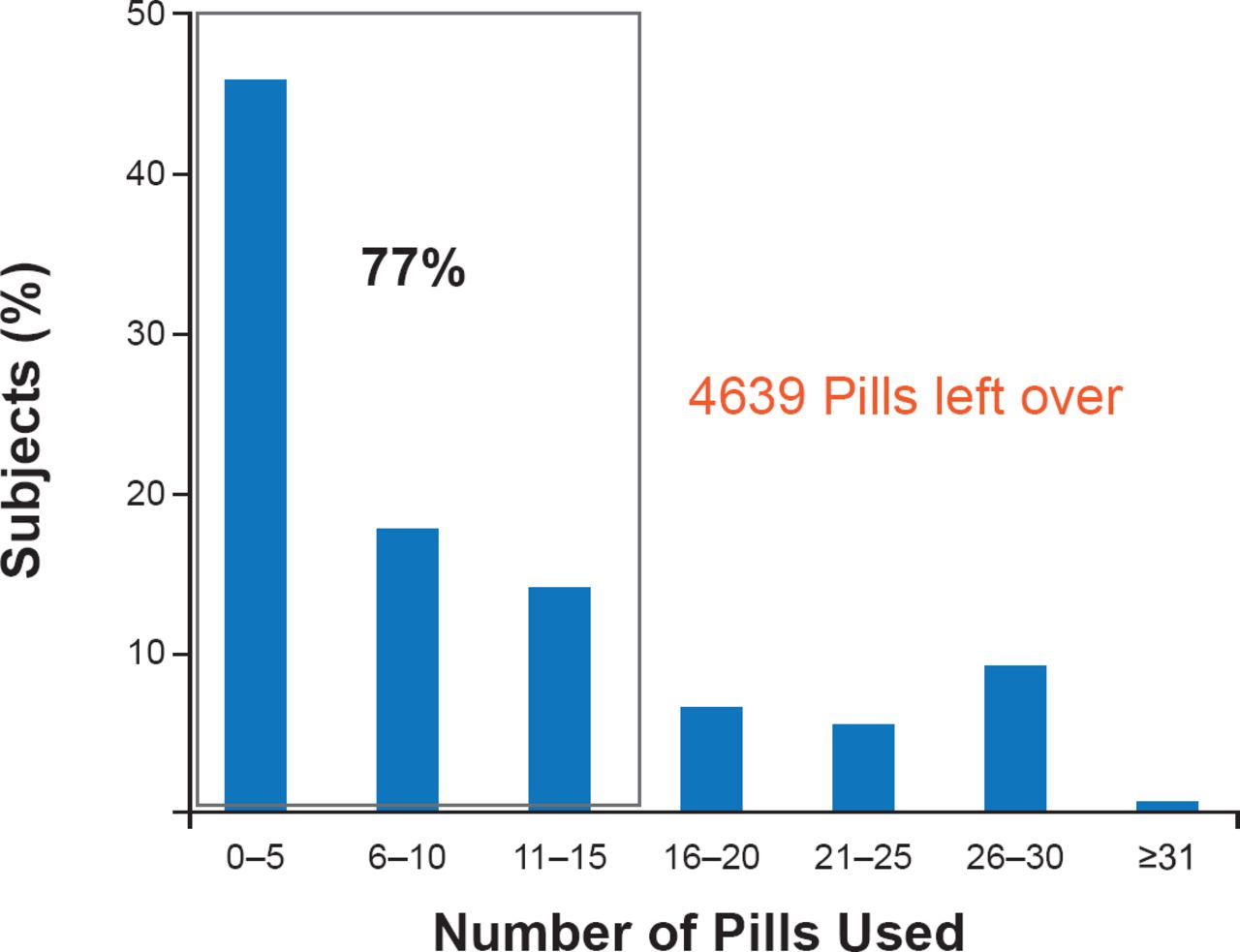
About 43% of patients did not use any over-the-counter analgesics, ∼32% used nonsteroidal anti-inflammatory drugs, and ∼13% used acetaminophen. Most (52%) patients used their prescribed medication on Days 0 to 2. The mean number of opioid pills used was 10, leaving >4600 pills unused (Figure 2). Medicaid patients used more opioids (25 pills) and Medicare patients used significantly less (7 pills; p<0.05) compared with private insurance and workers compensation patients.

Pill Usage Following Outpatient Surgery
Reproduced from Rodgers J et al. Opioid Consumption Following Outpatient Upper Extremity Surgery. J Hand Surgery 2012. With permission from Elsevier.
Limitations of the study are underreporting by patients, unaccounted procedural complications or postoperative infection, and type of anesthesia.
The policy of this orthopedic practice now is to prescribe 15 pills of a Schedule III opioid analgesic with one refill. They estimated that 23% of patients would require a refill. More importantly, said Dr. Rodgers, this would lead to a 79% reduction in leftover medication that could be diverted to persons for whom it was not prescribed, which is a leading source of opioids. He also said a prescription with more pills for hard tissue procedures and fewer pills for Medicare patients may be considered.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.