

Summary
This article discusses the substantial impact of obesity for hospitals, orthopedic practices, and individual patient outcomes, as well as measures to address these challenges. Special issues include anesthesia management pre- and intra-operatively, adapting surgical techniques, infection control, pain management, and hospital equipment.
- Orthopaedic Pain Management
- Obesity
- Cardiometabolic Disorder
- Orthopaedic Procedures
- Arthritis
- Orthopaedics
- Orthopaedic Pain Management
- Obesity
- Cardiometabolic Disorder
- Orthopaedic Procedures
- Arthritis
The substantial impact of obesity for hospitals, orthopedic practices, and individual patient outcomes, as well as measures to address these challenges, was discussed in this session moderated by George V. Russell, Jr, MD. Special issues include anesthesia management pre-and intra-operatively adapting surgical techniques, infection control, pain management, and hospital equipment.
A firm message from Mary I. O'Connor, MD, Mayo Clinic, Jacksonville, Florida, USA, is that blaming the patient for being obese will not help that individual lose weight. She notes that while personal responsibility remains a critical issue, there are powerful mediators which can make it very difficult for an individual to lose weight. Such mediators include culture, physical environment, economics, genetics, previous and current health status, and psychosocial factors.
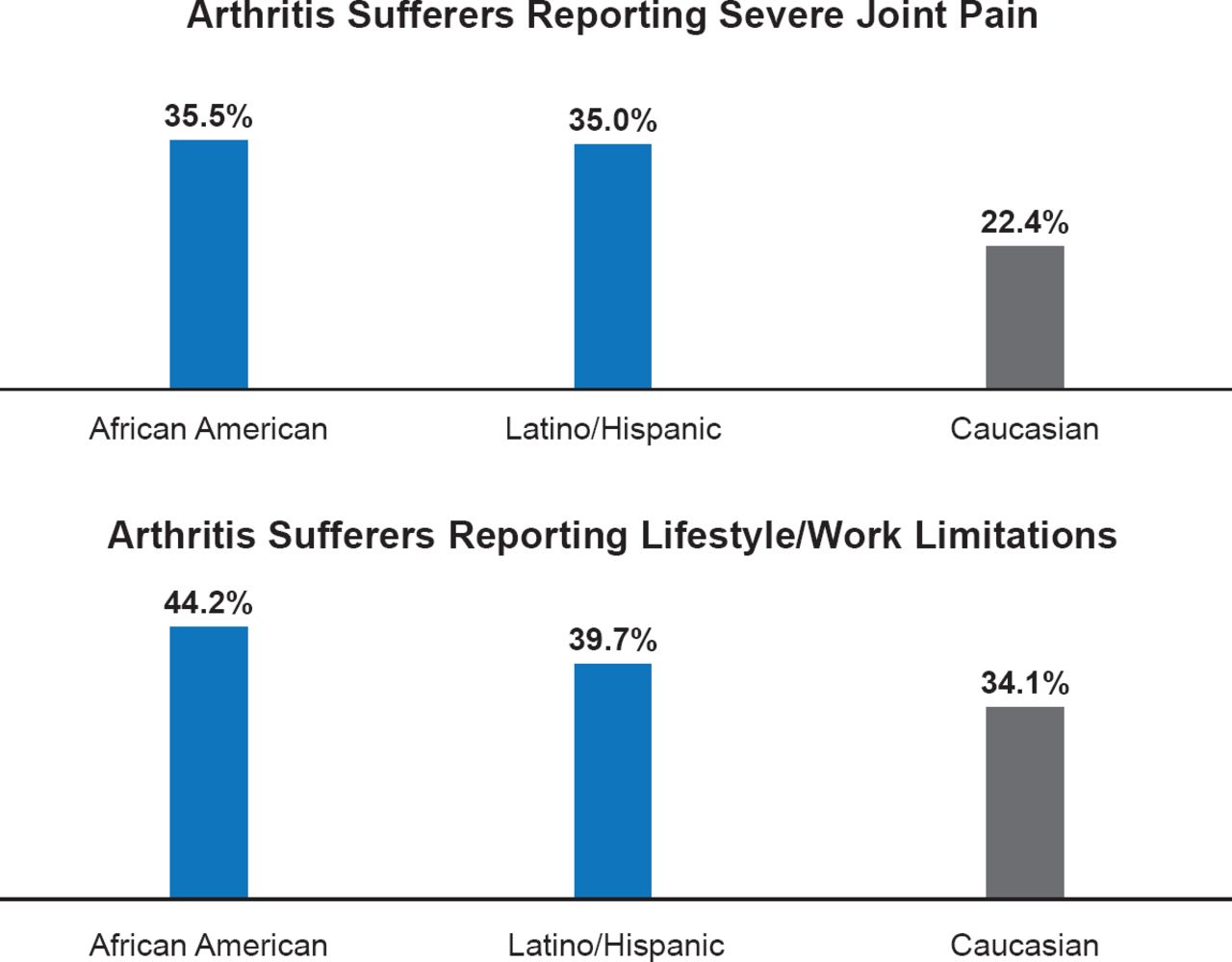
Dr. O'Connor highlighted that effective dialogue regarding obesity and arthritis-related complaints should discuss differences related to race, ethnicity and gender. African Americans, Hispanics, and Mexican Americans have higher rates of obesity than Caucasians and within these groups women are more obese than men. Only in Caucasians is the obesity rate higher in men compared with women (Figure 1). The relationship between obesity and arthritis is strong; overall, the rate of arthritis is 58% higher in women than in men.

Ethnic and Racial Disparities for Rates of Arthritis Complaints
Source: National Health Interview Survey 2002.
Patient motivation to lose weight remains critical, and behavioral science is providing new insights into effective strategies. These include patient discovery (weighing themselves), patient-centered benefits (increased energy motivates ongoing weight loss), referral to a behavior change expert, and the use of community resources such as Weight Watchers to support lifestyle change. Patient motivation is strongly impacted by culture, which influences not only how weight is viewed by the individual but also the preferred type of help for weight loss. African American females want encouragement from their primary care physician, group meetings with their healthcare team, and other women, while Caucasian females prefer individual weekly meetings with a primary care physician [Blixen CE et al. J Natl Med Assoc 2006]. Weight loss interventions that work for Caucasians are not as effective for Hispanics and Latinos [Lindberg NM, Stevens VJ. Ethn Dis 2007]. Dr. O'Connor notes that much more research is needed to develop effective weight loss strategies and that these need to be tailored to the race/ethnicity/gender of the obese patient.
MANAGING COMORBIDITIES IN OBESITY IN THE SURGICAL SETTING
Obese patients are at higher risk for surgical complications. Obesity is associated with other comorbidities and the cumulative effect of these further increases the risk of complications and poor outcomes after surgery, said William M. Mihalko, MD, PhD, Campbell Clinic Department of Orthopaedic Surgery & Biomedical Engineering, University of Tennessee Health Science Center, Memphis, Tennessee, USA.
The metabolic syndrome (MetS)—presence of obesity and ≥2 other comorbidities (hypertension, dyslipidemia, or diabetes)—is an independent risk factor for major complications, nonroutine discharge, and increased hospital cost after elective hip and knee arthroplasty [Gonzalez Della Valle A et al. J Arthroplasty 2012] and for increased in-hospital complications after traumatic isolated ankle fracture (OR, 2.1) [Menendez ME et al. Foot Ankle Intl 2014]. In lumbar spine fusion surgery, MetS significantly increased hospital stay, hospital charges, rate of major life-threatening complications, and nonroutine discharge [Memtsoudis SG et al. Spine (Phila Pa 1976) 2012].
Diabetes and glucose control before and during surgery affects outcomes. Poor glucose control is associated with risk of surgical site infection (SSI). One study showed that 90 of 318 (28.3%) patients with diabetes had complications after orthopedic surgery [Lamloum SM et al. Med Princ Pract 2009]. It also showed that good glucose control (HbA1C <7%) was significantly associated with a decreased risk of infection, while poorer control (HbA1C ≥7%) significantly increased urinary tract infections and SSI. A retrospective cohort study of 13,800 patients showed preoperative hypoglycemia and glucose variability was associated with in hospital death [Jeon CY et al. PLoS One 2012]. Perioperative hyperglycemia (≥2 blood glucose levels ≥200 mg/dL) was an independent risk factor for 30-day SSI in orthopedic trauma patients with or without diabetes in another study [Richards IE et al. J Bone Joint Surg Am 2012].
Peripheral neuropathy and peripheral vascular disease are twice as likely to occur in obese than in nonobese patients [Ylitalo KR et al. Diabetes Care 2011]. Revision arthroplasty was needed sooner in obese than in nonobese patients (average 79.2 vs 99.0 months; p=0.036) and they had significantly lower improvement in function scores at 6 months in the North American Knee Arthroplasty Revision study [Mulhall KJ et al. J Knee Surg 2007].
Obstructive sleep apnea (OSA) also increases surgical risk in obese patients with perioperative complications, and is higher in ambulatory surgery patients regardless of whether general or regional anesthesia is administered [Stierer TL et al. J Clin Sleep Med 2010].
CONSIDERATIONS FOR ANESTHESIA IN MORBIDLY OBESE PATIENTS
Patients with morbid obesity (body mass index [BMI] ≥40 kg/m2) have high surgical risk, requiring careful consideration of unique issues, beyond the usual assessment and care, including OSA, airway anatomy, ventilation and intubation, vascular access, pain management, and postoperative complications, which were reviewed by Kenneth Oswalt, MD, University Medical Center, Jackson, Mississippi, USA.
Beyond the usual cardiovascular assessment, the presence of obesity cardiomyopathy, arrhythmias, and ischemic heart disease must be identified. Ventricular function should be assessed by echocardiography, because dysfunction will require invasive testing by a cardiologist.
Airway management is a concern because of OSA, which Dr. Oswalt assumes is present in all morbidly obese patients, and reduced pharyngeal area. Notably, neck obesity is more important than generalized obesity to determine the risk of OSA, he said. Regional anesthesia, close monitoring of the airway during surgery and pulse oximetry after surgery, and minimal use of opioids is recommended.
Intraoperative issues are access (airway, intravenous), anesthesia choice, and accommodation (patient positioning). Approaches to address difficult ventilation and intubation are shown in Table 1. Pulmonary atelactasis can be addressed by positive end-respiratory pressure and raising the head of bed by 30 degrees to increase residual functional capacity. Venous access is improved with ultrasound guidance, which is now the gold standard for central line placement.
Strategies to Address Difficult Ventilation and Intubation
Factors affecting anesthesia selection are patient size and body habitus, coexisting history and comorbidities, type of surgical procedure, skill and preference of anesthetist, and preference of surgeon and patient. Objectives of anesthesia maintenance in the obese are outlined in Table 2.
Objectives of Anesthesia Maintenance in Obese Surgical Patients
Pain management is critical in obese patients to help mobilize them postoperatively. Of note, obese patients are more sensitive to the respiratory depressant effects of opioids, requiring cautious use and close monitoring.
Close observation is required in the postanesthesia care unit, especially of oxygen saturation, and use of continuous positive airway pressure machines should be resumed. Ventilation abnormalities are exacerbated and may last days in these patients. Care is required for the timing of discharge of patients with obesity and OSA, because the maximum decrease in partial pressure of arterial oxygen occurs on postoperative Day 2 or 3.
INTRAOPERATIVE MANAGEMENT OF OBESE PATIENTS
An increasing BMI proportionally increases operative time and complications [Wang JL et al. J Arthroplasty 2013] and the risk of SSI [Namba RS et al. J Bone Joint Surg Br 2012]. Special considerations for antibiotics are time for adequate skin penetration, dose, dosing interval, and the lipophobicity of most prophylactic antibiotics, said William A. Jiranek, MD, Virginia Commonwealth University, Richmond, Virginia, USA. He recommends having the pharmacy calculate the dose and interval, because of the complexity to achieve the desired minimal inhibitory concentrations. Due to insufficient antibiotic concentrations in subcutaneous layers other strategies may be needed to fully protect the subcutaneous tissue, such as local administration of antibiotics (vancomycin powder), instilling diluted betadine or chlorhexadine, and pulsatile lavage. The Kaiser Permanente National Total Joint Replacement Registry showed a 50% decrease in infection with antibiotics added to surgical cement [Parvizi J et al. Acta Orthop 2008] in patients with BMI >35.
Patient positioning issues include a sufficiently large operating table (bariatric service, secure two standard tables together) to hold the weight of the patient and ensure no falls, arranging the panniculus to allow access for the incision, and larger positioning devices. Gel padding is needed to prevent pressure sores. Dr. Jiranek advised draping the patient generously due to the need for longer skin incisions to create adequate deep exposure.
Incisions should avoid skin folds and adequate hemostasis is needed in the deep tissues. Longer retractors and longer, wider self-retainers are needed. Imaging is advised during surgery to avoid malposition and because direct visualization of bony landmarks is more difficult (the femoral insertion site for intramedullary devices and acetabular component abduction are two examples), and this requires advance planning for types of tables and positioning of radiographic equipment, and ensuring adequate imaging penetration.
Intraoperative foot pumps and preoperative anticoagulants should be employed to prevent deep vein thrombosis, because obese patients appear to be at increased risk Obese patients with MetS with long bone fractures or total joint replacement should be sent to the intensive care unit or stepdown monitoring because of the increased risk of death from fat embolus as well as other cardiac and pulmonary complications after orthopedic surgery. Regarding surgical closure, a reinforcing layer in the subcutaneous layer is recommended because of the risk of wound dehiscience, and a wound vacuum should be considered.
Abdominal girth leads to positioning difficulties, pressure sores, and ventilation concerns, and body size may require changing a surgeon's preferred technique, said George V Russell, Jr, MD, University Medical Center, Jackson, Mississippi, USA. Complications in obese patients are similar to nonobese patients who undergo appendicular skeleton surgical procedures, but they have more wound complications with axial skeleton surgery and wound and systemic complications with polytrauma surgery. Wound complications, especially related to trauma surgery, can be sufficiently substantial and lead to necrotic tissue that must be removed.
RESTRICTED ACCESS TO SURGERY FOR OBESE PATIENTS
The risk-benefit ratio of surgery in obese patients is difficult to calculate, and the threshold at which the higher risk outweighs the probability of success is not clear. However, financial pressures may lead physician practices and hospitals to limit access to surgery for obese patients, because new approaches to reimbursement (value-based payment, bundling, accountable care organizations, others) may not cover the actual costs of these patients who have higher rates of complications and rehospitalization, said Adolph J. Yates, Jr, MD, University of Pittsburgh, Pittsburgh, Pennsylvania, USA. He noted that obese patients are not the only category who may face such discrimination. To address this issue, improved risk adjustment tools are needed, along with improved data (appropriate coding, databases, registries), and excluding certain categories of patients from value reporting and new modes of payment, said Dr. Yates.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.