

Summary
Although BRCA1 and BRCA2 mutations are not common, their presence confers a high risk of developing breast or ovarian cancer. This article presents current preventative measures for breast and gynecologic cancers as a result of BRCA1 and BRCA2 mutations.
- Oncology Genomics
- Reproductive Cancers
- Breast Cancer
- Oncology Genomics
- Reproductive Cancers
- Obstetrics & Gynecology
- Breast Cancer
Although BRCA1 and BRCA2 mutations are not common, their presence confers a high risk of developing breast or ovarian cancer. Noah D. Kauff, MD, of Memorial Sloan-Kettering Cancer Center, New York, New York, USA, presented current preventative measures for breast and gynecologic cancers as a result of BRCA1 and BRCA2 mutations.
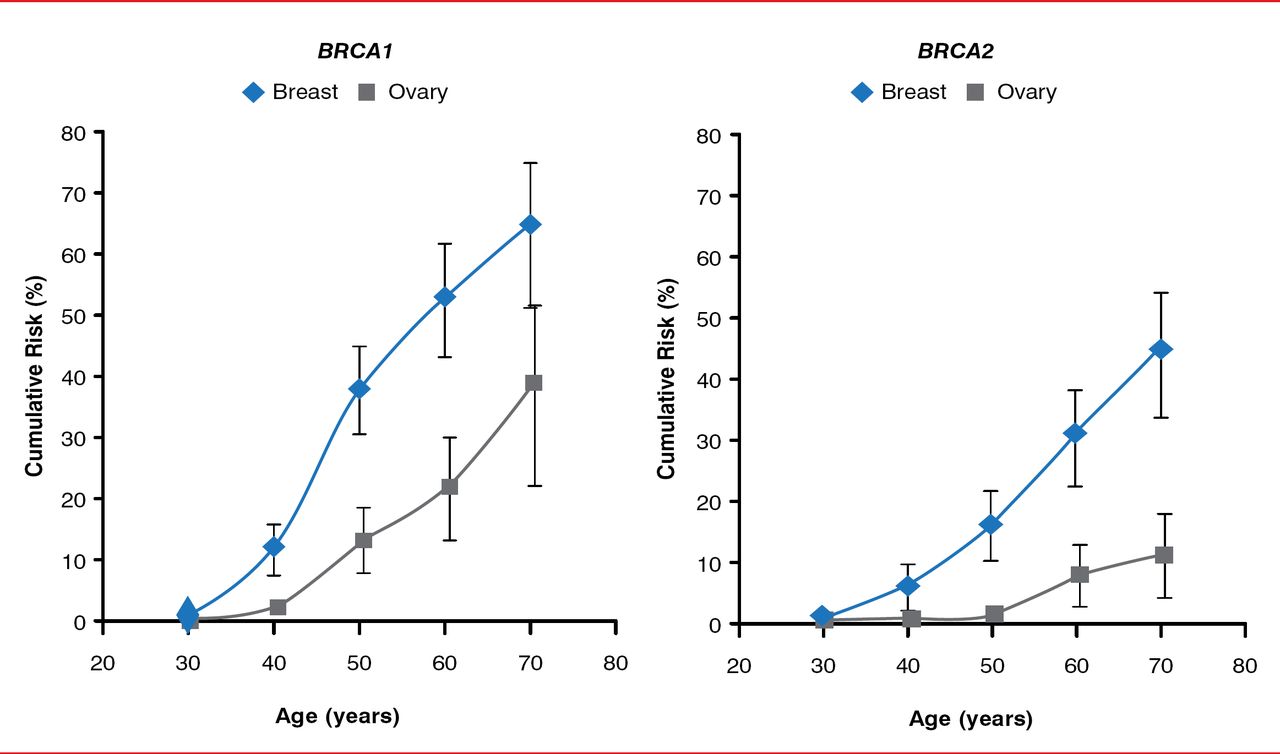
Breast, uterine, and ovarian cancers are among the top 5 most common cancers in women. Up to 10% of these are associated with a single gene mutation. A common cancer susceptibility syndrome is hereditary breast and ovarian cancer, in which the BRCA1 or BRCA2 gene is mutated. Patients with BRCA1 mutations have up to a 25% risk of estrogen receptor (ER)-positive breast cancer and up to a 46% risk of ovarian cancer, whereas patients with BRCA2 mutations have up to a 79% risk of ER-positive cancer and up to a 27% risk of ovarian cancer (Figure 1) [Antoniou A et al. Am J Hum Genet 2003; King MC et al. Science 2003].

Cumulative Risk Estimates for Patients With BRCA Mutations
Reproduced from Antoniou A et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet 2003;72(5):1117–1130. With permission from Elsevier.
Patients with confirmed BRCA mutations should undergo intensive surveillance, receive chemoprevention, and/or undergo risk-reducing surgery to prevent breast and ovarian cancer. Mammography is estimated to have a 42% to 56% sensitivity in patients with BRCA mutations, with the ability to detect lymph node metastases in 25% to 56% of patients [Brekelman et al. J Clin Oncol 2005; Scheuer L et al. Clin Oncol 2002]. However, magnetic resonance imaging (MRI) has been demonstrated to have greater sensitivity than mammography for the detection of breast cancer (Table 1) [Leach MO et al. Lancet 2005]. In addition, MRI is more sensitive at detecting breast cancer in earlier stages when compared to mammography [Warner E et al. J Clin Oncol 2011].
Enhanced Sensitivity for Breast Cancer Detection With Magnetic Resonance Imaging
Chemoprevention with tamoxifen can be offered to women with a 5-year projected risk of breast cancer of ≥1.66%; however, there is no overall health or survival benefit [Visanathan K et al. Clin Oncol 2013]. In patients with BRCA mutations, use of oral contraceptives and increased duration of use are associated with a decreased risk of ovarian cancer [Moorman PG et al. Clin Oncol 2013; Cibula D et al. Expert Rev AntiCancer Ther 2011].
Risk-reducing surgery results in a clear decrease in the risk of developing breast or ovarian cancer when compared with surveillance alone [Domchek SM et al. JAMA 2010; Kauff ND et al. N Engl J Med 2002; Rebbeck TR et al. N Engl J Med 2002]. Interestingly, Dr. Kauff highlighted that, when carrying out risk-reducing surgery, it is essential to isolate the ovarian blood supply and to ligate it distal to its insertion into the ovary in order to reduce the risk of primary peritoneal cancer in the event that an ovarian remnant remains. In addition, there is a question as to whether a concomitant hysterectomy should be performed with risk-reducing salpingo-oophorectomy (RRSO). Advantages of this approach include ensuring the removal of the entire fallopian tube and eliminating the risk of uterine cancer, whereas the disadvantages include a higher risk of complications and increased operating time and cost.
Patients with BRCA mutations who wish to have children have several fertility preservation options, including natural conception with limited breast feeding and continued surveillance, embryo/oocyte cryopreservation for future in vitro fertilization followed by RRSO, and risk-reducing mastectomy with RRSO in the mid-40s.
Dr. Kauff concluded by highlighting the challenges of identifying individuals at risk of breast and gynecologic cancers, and he stated that he was hopeful that advances in chemoprevention may one day render risk-reducing surgery obsolete.

The editors would like to thank the many members of the 2014 American Congress of Obstetricians and Gynecologists presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.