

Summary
This article discusses drug therapy in mood disorders, recent developments in anxiety, updates in obsessive-compulsive disorder therapy, as well as neural mechanisms of fear in posttraumatic stress disorder (PTSD).
- Psychopharmacology
- Mood Disorders
- Anxiety Disorders
- Psychopharmacology
- Psychiatry
- Mood Disorders
- Anxiety Disorders
A cadre of researchers from Columbia University Medical Center, New York City, New York, USA, provided a clinical and research update on anxiety, eating, and mood disorders.
DRUG THERAPY OF MOOD DISORDERS
Patrick J. McGrath, MD, discussed recent advances in drugs used in the treatment of mood disorder. Selected diagnostic revisions from the recently updated Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) has absorbed dysthymia as part of persistent depressive disorder (PDD), which features the absence of mania, hypomania, and cyclothymia. Individuals diagnosed with PDD experience depression more days than not and have two or more of poor appetite or overeating, insomnia or hypersomnia, low energy or fatigue, low self-esteem, and poor concentration or indecisiveness.
An anxious distress modifier has been added to all mood disorders to recognize that this predicts a somewhat poorer response to selective serotonin reuptake inhibitor (SSRI) antidepressants. The “with anxious distress” modifier features the presence of some or all of five symptoms (Table 1) during the majority of days: mild, two symptoms; moderate, three symptoms; moderate-severe, four or five symptoms; severe, four or five symptoms along with motor agitation.
Symptoms of Anxious Distress
Levomilnacipran is a new serotonin norepinephrine reuptake inhibitor (SNRI). An enantiomer of milnacipran, it is more pharmacologically active and is a relatively potent inhibitor of the norepinephrine transporter. The interest of this potency is that it may be more effective for some dimensions of depression like attention, working memory, concentration, alertness, energy, and social activity than are medications more selective for serotonin reuptake blockade. The drug is administered for treatment of major depressive disorder at a dose of 20 mg/day, increased to 40 mg/day at first and ultimately (if tolerated) to 120 mg/day in 40-mg increments. Food has no effect on drug absorption.
Vortioxetine is an SSRI with agonist, partial agonist, or antagonist action, depending on the serotonin receptor binding site. Vortioxetine appears to have beneficial effects on cognition according to animal models, which could be advantageous for some patients. The most common adverse effect is nausea (about one-quarter to one-third of users), which is typically mild and occurs in the first week of treatment. The drug is initially given at a dose of 10 mg/day with subsequent increase to 20 mg/day if tolerated. Dose-related benefits have been documented. Food has no effect on drug absorption.
Lurasidone is a newly FDA-approved treatment for bipolar depression. Although clearly effective, its tolerability with long-term use is a concern, as are the sedative effect and weight gain. A recent 6-week, randomized, double-blind, placebo-controlled study of lurasidone monotherapy in the treatment of bipolar I depression demonstrated the drug's efficacy compared with placebo (n= 162), with no dose response evident when using 20 to 60 mg/day (n=161) and 80 to 120 mg/day (n=162) [Loebel A et al. Am J Psychiatry 2014].
Interest is building in the use of ketamine in the relief of depression. Recent results of a two-site, randomized control trial that compared Montgomery-Asberg Depression Rating Scale (MADRS) scores after 24 hours (primary outcome) and for up to 7 days for 47 subjects receiving ketamine and 25 subjects receiving placebo reported that ketamine use met the primary outcome, with the significant improvement persisting to 7 days [Murrough JW et al. Am J Psychiatry 2013]. The ketamine-treated subjects also displayed a significantly higher response rate, measured using the MADRS, on Days 1, 2, 3, and 7. Ketamine studies have raised the possibility of developing faster acting, and more effective antidepressant treatments using modulation of glutamate neurotransmission.
The Establishing Moderators and Biosignatures of Antidepressant Response for Critical Care study [EMBARC; NCT01407094] is now underway, aimed at clarifying the optimal treatment for depression based on individual biology. Its goal is to develop biosignatures of specific antidepressant responses using brain imaging, electrophysiology, and behavioral testing, ultimately to be able to select antidepressant medication treatment rationally rather than through a process of trial and error.
ANXIETY
Franklin Schneier, MD, reviewed recent developments in anxiety. Fear is an emotion related to an immediate response to an actual threat, and mobilizes the “fight or flight” response. Anxiety is an emotion related to an anticipation of threat, and drives preparative or avoidance strategies. Anxiety is an evolutionary trait that is valuable for survival. But anxiety that is disproportionate or inappropriate to the particular circumstance is the hallmark of anxiety disorder. It is the most common class of psychiatric disorders, with >20% of all individuals being affected in their lifetime. Aside from the human cost, the economic costs are enormous, with estimates of $42 to $47 billion in health care system expenditures, representing 30% and 53% of total and drug expenditures for mental illness, respectively [Ohayon MM. J Psychiatr Res 2006].
The DSM-5 includes the two new anxiety disorders that were previously recognized as disorders occurring only in children: separation anxiety disorder (distress concerning separation from attachment individuals, such as parents, or spouse or child) and selective mutism (failure to speak in certain situations while speaking normally in others).
Panic disorder, phobias, and generalized anxiety disorder are anxiety disorders that share a chronologically early onset and often become chronic. These disorders are more prevalent in women by a 2:1 margin. All exact appreciable social and occupation disabilities and can be risk factors for depression, alcohol abuse, and suicide. The good news is that efficacious treatments are available. The bad news is that these treatment options continue to be underutilized.
Cognitive behavioral therapy (CBT) is an evidence-based psychotherapy that has been adapted to treat specific anxiety disorders. The benefits of CBT can sometimes surpass those attained using medications. Medications used as first-line drugs include selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors. There is no evidence of superiority of any particular SSRI or SNRI. Alternatives to SSRIs, based on evidence from randomized controlled trials, are benzodiazepines, buspirone, pregabalin/gabapentin, tricyclics, β-blockers, and monoamine oxidase inhibitors although only a subset has specific FDA indications for anxiety disorders.
OBSESSIVE-COMPULSIVE DISORDER
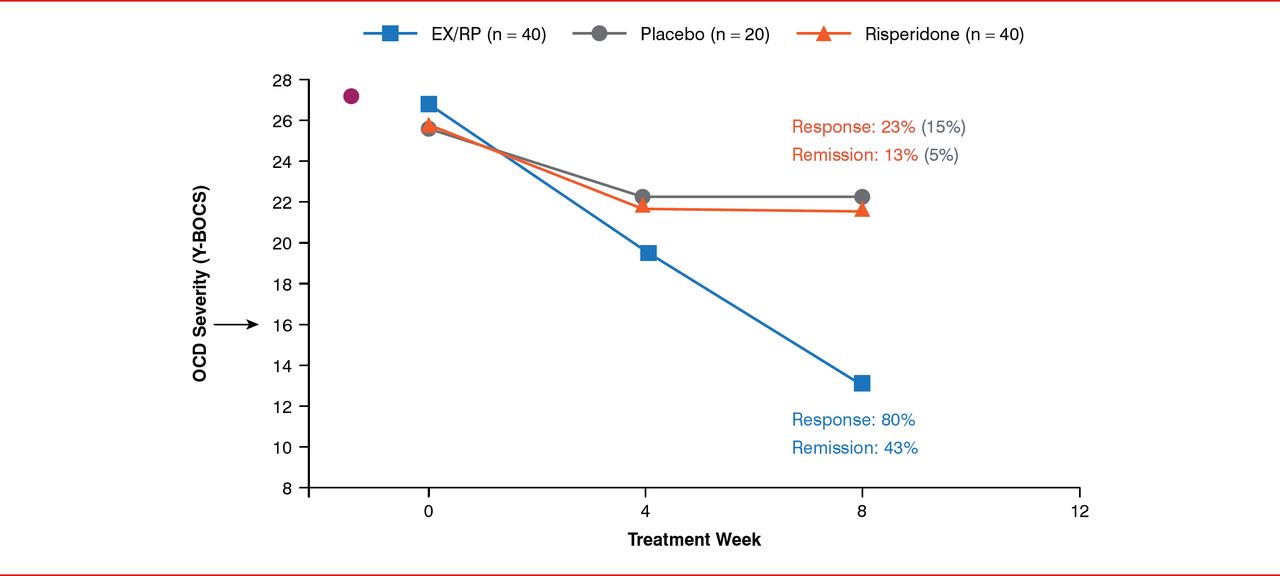
According to Helen Blair Simpson, MD, PhD, obsessive-compulsive disorder (OCD) is a disabling disorder with a lifetime prevalence of approximately 2% following its onset—half of cases start by age 19, with a quarter starting by the age of 14 [Kessler RC et al. Arch Gen Psychiatry 2005]. The onset age is considerably younger than for major depression, for which 50% of cases start by 32 years of age [Kessler RC et al. Arch Gen Psychiatry 2005]. OCD is chronic, often with a “waxing and waning” pattern of occurrence. OCD and obsessive-compulsive personality disorder (OCPD) are both impairing disorders marked by ritualized behaviors but are differentiated by the presence of obsessions in OCD and by excessive capacity to delayreward in OCPD [Pinto A et al. Biol Psych 2014]. Treatments for OCD include the tricyclic antidepressant clomipramine, various SSRIs (including fluoxetine, fluvoxamine, sertraline, paroxetine, Citalopram and escitalopram, all of which are FDA approved for OCD, and Citalopram and escitalopram, which are not FDA approved for OCD), and CBT consisting of exposure and ritual (or response) prevention (EX/RP). In one study, EX/RP combined with clomipramine (n=31) and EX/RP alone (n=29) significantly reduced OCD severity compared with clomipramine alone (n=36) group and the placebo (n=26) group after 12 weeks of treatment [Foa EB et al. Am J Psychiatry 2005]. EX/RP can augment SRIs (ie, clomipramine and the SSRIs), with response rate and rate of symptom remission for EX/RP augmentation to be 74% (40/54) and 33% (18/54), respectively, as compared to augmentation with stress management therapy of 33% (18/54) and 4% (2/54), respectively. [Simpson HB et al. Am J Psychiatry 2008]. EX/RP augmentation of SSRIs was also superior to antipsychotic augmentation with risperidone (Figure 1) [Simpson HB et al. JAMA Psychiatry 2013].

Augmenting SRIs: EX/RP and Antipsychotics
EX/RP=exposure and ritual prevention; OCD=obsessive-compulsive disorder; SRI=serotonin reuptake inhibitor; Y-BOCS=Yale-Brown Obsessive Compulsive Scale.
Reproduced from Simpson HB et al. Cognitive-Behavioral Therapy vs Risperidone for Augmenting Serotonin Reuptake Inhibitors in Obsessive-Compulsive Disorder: A Randomized Clinical Trial. JAMA Psychiatry 2013;70(11):1190–1199. With permission from the American Medical Society.
For the patients of tomorrow, development of novel treatments, such as ketamine [Rodriguez CI et al. Neuropsychopharmacology 2013], based on a better understanding of the underlying brain mechanisms, should lead to identification of new treatment targets.
POSTTRAUMATIC STRESS DISORDER
Yuval Neria, PhD, discussed neural mechanisms of fear in posttraumatic stress disorder (PTSD). Traumatic events are common, with more than half of American men and women experiencing at least one such event in their lives. Yet, only a minority develops persistent PTSD, which has prompted the hypothesis that PTSD involves a failure of neural mechanisms of recovery [Yehuda R, LeDoux JE. Neuron 2007].
Efforts to clarify these neural mechanisms are utilizing functional magnetic resonance imaging, skin conductance response, and clinical assessments. The ultimate goal is to identify neural predictors of treatment response. PTSD research is focusing on the early neural events in fear conditioning, late extinction, and extinction recall [Amstadter AB et al. Psychiatr Ann 2009]. Emerging data suggest that deficits in the ability to recall extinction memory are associated with PTSD and fear circuitry, including the hippocampus and ventromedial cortex [Milad MR et al. Biol Psychiatry 2009; Shvil E et al. Neurobiol Learn Mem 2014]. Whether deficits in extinction recall can be reversed and relevant psychotherapy is appropriate to induce changes in brain functioning are open questions.
In prolonged exposure (PE) therapy, a patient's recollection of the traumatic event provides the springboard for assembling a list of activities that are better avoided or that provoke stress. Such an extinction-based approach may help a patient overcome the trauma of past events, which, in the brain, could involve reversal of dysfunctional circuitry in locations that perhaps include the prefrontal context and hippocampus that elicits the fear. Preliminary findings from a National Institute of Mental Health study (Yuval Neria, primary investigator) suggest that patients who clinically responded to PE therapy exhibited substantial improvement in their capacity to recall fear extinction, demonstrating enhanced activation of circuits involved in top-down control of fear processing including the hippocampus and the venro medial prefrontal cortex.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.