

Summary
Essential tremor, the most common movement disorder, occurs in =3.9% of the population, with tremor amplitude and associated disability increasing with age [Elble RJ. Neurology 2000]. Treatment is important because tremor can cause disability or social embarrassment, and many patients change jobs or retire as a result of essential tremor. This article discusses the medical therapy of essential tremor, the use of invasive and experimental therapies for the treatment of essential tremor, and management of rare tremors.
- Extrapyramidal & Movement Disorders
- Neurology
- Extrapyramidal & Movement Disorders
Essential tremor, the most common movement disorder, occurs in ≤3.9% of the population, with tremor amplitude and associated disability increasing with age [Elble RJ. Neurology 2000]. Treatment is important because tremor can cause disability or social embarrassment, and many patients change jobs or retire as a result of essential tremor. Tiago A. Mestre, MD, MSc, Ottawa Hospital, Ottawa, Ontario, Canada, discussed the medical therapy of essential tremor.
The β-adrenergic blocker propranolol has been evaluated in 13 studies as monotherapy or add-on treatment for essential tremor. With a mean effective dose of 60 to 240 mg/day for 2 to 12 weeks, propranolol has been shown to improve clinical severity rating, task performance, activities of daily living (ADL) measures, patient perception of change, and accelerometry data. Side effects include bradycardia and bronchospasm. A placebo-controlled randomized trial that compared propranolol versus long-acting propranolol found similar efficacy between the agents. Similarly, atenolol and sotalol were evaluated in 1 study each, and both showed efficacy.
Evaluation of primidone in 9 studies as a monotherapy and add-on treatment with a mean effective dose of >150 to 750 mg/day for 3 to 5 weeks showed improvement in clinical severity rating, task performance, and ADL measures. However, acute toxic reactions can occur, and the discontinuation rates ranged from 7.5% to 42%. Topiramate was evaluated in 4 studies as monotherapy and add-on treatment with a mean effective dose of 215 to 333 mg/day for 2 to 24 weeks and resulted in improved tremor amplitude and ADL measures in all but 1 study. Side effects included paresthesias, nausea, cognitive difficulties, and weight loss. As evaluated in 3 studies, gabapentin treatment as monotherapy or add-on with a mean effective dose of 1200 to 1800 mg/day for 2 to 6 weeks produced mixed results; 2 studies found improvement or modest effect, and 1 study found no effect.
Alprazolam, a benzodiazepine, was shown to reduce the severity of essential tremor and improve task performance and anxiety scores in 2 placebo-controlled studies. It was used as monotherapy with an effective dose of 0.75 to 1.5 mg/day. Side effects included somnolence in ≤50% of patients and risk of dependence.
In 2 studies, a dose of 50 to 100 U of botulinum toxin type A resulted in an improvement in tremor severity in patients with essential tremor that was refractory to oral medical therapy. In 1 of the studies, the effect was maintained for 16 weeks without impairing function. The main adverse event was dose-dependent arm weakness.
Although agents such as progabide, trazodone, mirtazapine, and amantadine are generally well tolerated, they are unlikely to be useful in clinical practice. Agents that have been found to be inefficacious include levetiracetam, and agents that remain investigational because of due to a lack of evidence include nadolol, olanzapine, clonidine, nimodipine, theophylline, flunarizine, metoprolol, pregabalin, phenobarbital, zonisamide, T2000, methazolamide, and acetazolamide. Isoniazid was found in 1 study to have an unacceptable risk profile.
Jens Volkmann, MD, University Hospital of Wurzburg, Wurzburg, Germany, presented on the use of invasive and experimental therapies for the treatment of essential tremor. Thalamotomy can be effective in ≤93% of patients but can cause permanent neurologic deficits in ≤23% of patients with essential tremor. However, thalamic deep brain stimulation (DBS) is equally effective in reducing tremor scores, has less permanent adverse effects, and results in better functional outcomes than does thalamotomy [Schuurman PR et al. N Engl J Med 2000]. Thalamic DBS may be indicated in patients who have tremor that is refractory to medical therapy, is severe with a tremor rating score of 3 to 4, and is considered disabling, either physically or socially.
For essential tremor, a meta-analysis of 10 studies found that DBS reduced tremor by 60% to >90% [Deuschl G et al. Lancet Neurol 2011]. With regard to DBS and treatment of other types of tremor, DBS can result in 80% to 90% complete or nearly complete suppression of resting tremor in patients with Parkinson's disease (PD). However, DBS can unfortunately cause progression of other symptoms of PD, and long-term complications that are normally prevented by levodopa therapy are not prevented with DBS. Subthalamic nucleus DBS is effective in tremor-dominant PD and should preferentially be used in younger patients. Thalamic DBS has also been shown to be effective in tremors of multiple sclerosis. However, Prof. Volkmann pointed out that in this population, DBS should be used in patients who have little other neurologic impairment because multiple sclerosis is a progressive multisymptomatic disorder.
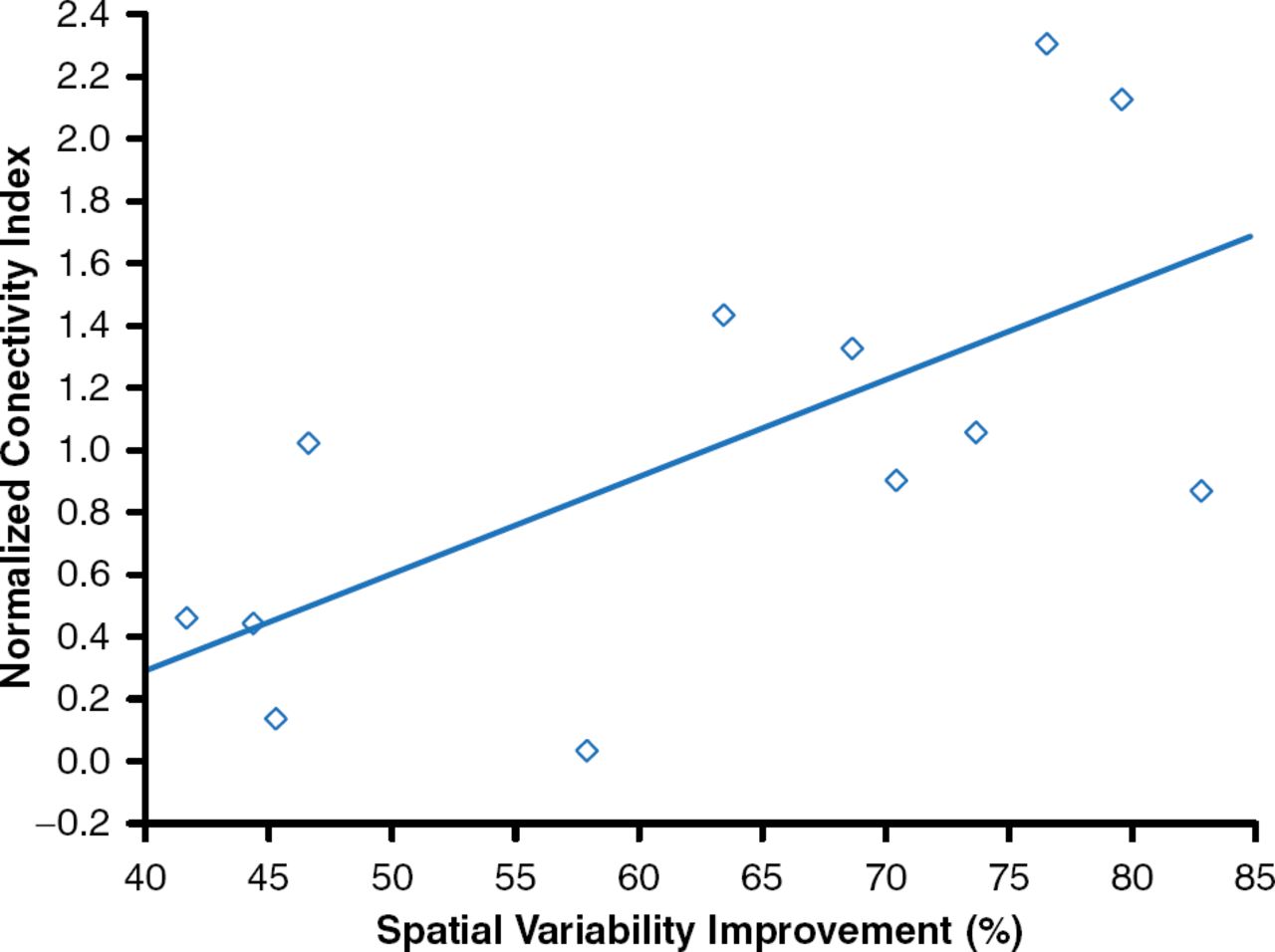
A more optimal target for thalamic DBS may be found on intention tremor when patients perform reach-to-grasp movements [Herzog J et al. Brain 2007]. In addition, DBS targeted near the dentate-thalamic tract results in improved outcomes of the procedure (r=0.660; p<0.05; Figure 1) [Groppa S et al. Brain 2014].

Effect of Deep Brain Stimulation Near the Dentate-Thalamic Tract
Reproduced from Groppa S et al. Physiological and anatomical decomposition of subthalamic neurostimulation effects in essential tremor. Brain. 2014;137(pt 1):109–121. With permission from Oxford University Press.
With regard to outcomes with DBS, thalamic DBS results in long-term (>5 years) improvements in refractory essential tremor, ADL score, and handwriting, but some complications can occur as well [Baizabal-Carvallo JF et al. J Neurol Neurosurg Psychiatry 2014]. Common complications include dysarthria and disequilibrium, particularly in patients who underwent bilateral stimulation, as well as hardware complications. In addition, this study noted that over time the efficacy of DBS decreases, likely due to the development of tolerance or progression of disease. In some patients, this deterioration of effect resulted in 5-year outcomes that were not better than thalamotomy [Schuurman PR et al. Mov Disord 2008]. In addition, 1 pilot study showed that magnetic resonance–guided focused ultrasound thalamotomy for the treatment of essential tremor resulted in improvement in tremor, disability, physical performance, and quality of life [Elias WJ et al. N Engl J Med 2013].
Marie Vidailhet, MD, PhD, Salpětrière University Hospital, Paris, France, discussed the management of rare tremors. Rarer tremor types can mimic essential tremor. For example, cortical myoclonic tremor with epilepsy causes distal tremulous movements, cortical hyperexcitability, and myoclonic or general seizures. Family case reports and small series have reported that the use of clonazepam, valproic acid, levetiracetam, and other antiepileptic drugs can reduce tremulous movements and seizures in this patient population. Additionally, utilizing gabapentin may induce myoclonus status [Striano P et al. Epilepsia 2007]. Another rare cause of tremor is damage to or structural abnormalities of the cerebellothalamocortical pathway [Sharifi S et al. Tremor Other Hyperkinet Mov (NY) 2012].
Myoclonus dystonia (MD) may mimic tremor and is characterized by mild dystonia and brief jerks that predominantly occur in the neck, trunk, or proximal upper limbs. The distinguishing features of MD include brief jerks of 25 to 256 milliseconds and lack of a cortical event before the jerk [Roze E et al. Neurology 2008]. There is insufficient evidence to support medical treatment of MD; however, some agents have shown a modest effect in some patients, including anticholinergics [Lee JH et al. J Clin Neurol 2011] and levodopa [Luciano MS et al. Mov Disord 2009]. Other studies have indicated that pallidal stimulation can result in long-term improvement in dystonia and myoclonus [Rughani AI, Lozano AM. Mov Disord 2013; Azoulay-Zyss J et al. Arch Neurol 2011; Gruber D et al. Mov Disord 2010].
Primary orthostatic tremor is characterized by a fast tremor (13 to 18 Hz) that affects the trunk and legs while standing. The tremor is intense and disabling, giving the patient a sense of unsteadiness and fear of falling. Similar to MD, there is no clear treatment for primary orthostatic tremor. Clonazepam may prove helpful in some patients at a dose of 1.2 to 8 mg/day; levodopa may also have efficacy in patients with secondary orthostatic tremor due to PD. Noninvasive as well as invasive stimulation of the cerebellothalamocortical network has been evaluated in very small studies and appears to show some degree of improvement [Yaltho TC, Ondo WG. Tremor Other Hyperkinet Mov (NY) 2011].
For patients with a psychogenic tremor, action tremor and resting tremor can also occur; however, distractibility and variability is present in 80% of cases [Gupta A, Lang AE. Curr Opin Neurol 2009; Hinson VK, Haren WB. Lancet Neurol 2006]. There is no standard treatment for these cases, although transcranial magnetic stimulation [Garcin B et al. J Neurol Neurosurg Psychiatry 2013] and tremor retrainment [Espay AJ et al. Parkinsonism Relat Disord 2014] may result in improvement.
Other experimental treatments for tremor include gamma-knife thalamotomy, which has been evaluated for treatment of intractable tremors from PD and essential tremor and results in long-term improvement [Ohye C et al. Neurosurgery 2012; Young RF et al. J Neurosurg 2000]. Focused ultrasound thalamotomy has also resulted in improvement, as Prof. Volkmann mentioned earlier in the session [Chang JW et al. J Neurol Neurosurg Psychiatry 2014; Elias WJ et al. N Engl J Med 2013].
In conclusion, DBS and thalamotomy can provide good results in patients with PD or essential tremor. In rare tremor types, there is no clear medical therapy that substantially reduces symptoms; however, evaluation of brain stimulation has shown promise.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.