

Summary
Failed midfoot repairs can occur as a result of anatomic, patient, mechanical, and technical factors. This article discusses failed reconstructions, misaligned midfoot reconstruction, and the management of missed midfoot injuries.
- Orthopaedic Procedures
- Foot & Ankle Conditions
- Orthopaedic Procedures
- Orthopaedics
- Foot & Ankle Conditions
Failed midfoot repairs can occur as a result of anatomic, patient, mechanical, and technical factors. Jeffrey E. Johnson, MD, Barnes-Jewish Hospital at Washington University, St Louis, Missouri, USA, discussed the impact of these issues and others when managing failed reconstructions.
The midfoot is prone to problems for a variety of reasons. It is composed of multiple small bones that have a surface area too small for fusion; large areas of the bones are covered in cartilage that has limited blood supply; and the thin dorsal soft tissue envelope that encloses the midfoot is associated with poor wound healing and limits hardware options and incision placement. In addition, because the midtarsals can only be accessed dorsally, intraoperative joint preparation is difficult. Patient factors (eg, bone loss, osteopenia, prior procedures, smoking, noncompliance with non-weight-bearing, and comorbidities such as diabetes, inflammatory arthritis, and neuropathy) also contribute to the difficulties of the midfoot. Mechanical issues include stress from bending with weight-bearing and gastrocnemius-soleus contracture.
Before intervention, Dr Johnson assesses the midfoot with weight-bearing radiography, observes standing alignment, checks ankle/hindfoot range of motion, and performs a careful palpation to determine which joints are contributing to the pain and/or deformity. He may perform multiple and extended incisions to check for structures that might be in the way of exposure/fixation. Fusion techniques include cancellous bone impaction grafting, deformity correction by shortening and apposition, and lengthening with structural auto/allografts, which can correct for bone loss that is often present.
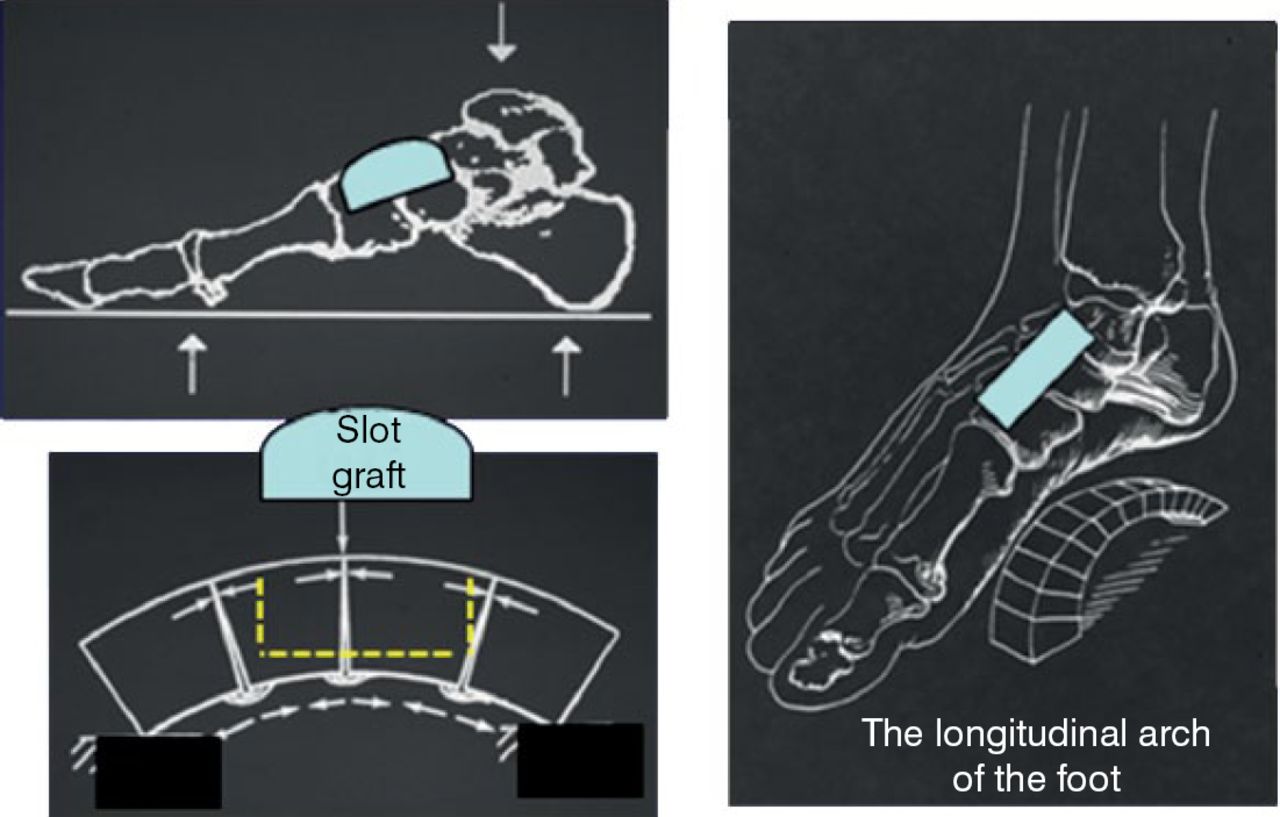
The slot graft technique is a successful (77% union) approach for midfoot fusions in high-risk patients. It is also associated with a low rate of complications, high patient satisfaction, and low pain scores (Figure 1) [Klein SE et al. Foot Ankle Int. 2011]. This technique may also improve rigidity of construct and fusion rate. Dr Johnson looks forward to new implants or plates that solve fixation problems and improve healing rates.

Midfoot Fusions With Dorsal Slot Graft
Reproduced with permission from JE Johnson, MD.
Brian C. Toolan, MD, The University of Chicago, Chicago, Illinois, USA, shared his experience with formulating an operative plan for reconstructing a misaligned midfoot due to a congenital or acquired deformity.
Correcting a deformity of the midfoot often requires managing a variety of challenges affecting the bone, joints, and soft tissues. Each challenge must be addressed, but the individual solutions must not interfere with one another or compromise the overall goal of achieving timely healing and a durable foot for weight-bearing. Dr Toolan often combines medial and lateral incisions on the dorsum of the foot with a medial-longitudinal incision to expose the midfoot for reconstruction.
The primary objective of his operative plan focuses on restoring the alignment of the longitudinal and transverse arches of the foot. He first considers the structural integrity and weight-bearing capacity of the 5 bones of the midfoot. Each bone is evaluated for its shape, continuity, and blood supply. Next, the joints are assessed for congruency, stability, and integrity of their articular cartilage. Weight-bearing radiographs and computed tomographic scans can assist in determining presence and severity of these factors for a particular joint. An equinus contracture of the ankle due to tightness of the gastrocnemius or Achilles tendon must be identified and eliminated in order to reduce excessive bending forces on the midfoot, which can undermine the outcome of the reconstruction. Tendon imbalances caused by atrophy or overpull of the posterior tibial and peroneus brevis muscles (due to atrophy or overpull of tendons) must be corrected to prevent an abduction or adduction deformity in the midfoot.
Dr Toolan recommends meticulous preparation for arthrodesis. He advises maintaining the peripheral cortical rim and avoiding the tendency to round or wedge the corners of the bones. Failure to maintain the proper shape and surface of the bones can affect alignment of the joint when the two are apposed for fusion. In addition, he pays close attention to re-establishing the keystone-mortise of the second tarsometatarsal joint in order to restore the longitudinal and transverse arches of the midfoot. He advises the use of bone grafting to increase the rate of successful fusion. Small or shallow defects at the periphery of a fusion can be patched with cancellous bone. Dorsal defects can be corrected with a small structural corticocancellous grafts. Major defects need structural grafts like a tricortical graft to support the arch.
Internal fixation of an arthrodesis should use crossed compression screws, preferably solid and stainless steel, with 2 screws per arthrodesis for stable, rigid fixation. Short screws and plates provide less resistance to bending and shear forces across a fusion, whereas longer screws or plates spanning the joint give more leverage to resist bending and avoid a loss of fixation and subsequent nonunion. Biological adjuvants such as platelet-rich plasma, mesenchymal stem cells, demineralized bone matrix, and porous tantalum may be used to supplement bone healing.
Postoperatively, a non-weight-bearing compressive splint or cast can be applied for the first 4 to 6 weeks while the reconstruction heals. This is followed by progression to full weight-bearing in a boot over 4 weeks with physical therapy for range of motion, resistive strengthening, gait training, and pool exercises. Once full weight-bearing is achieved, weaning to shoes with orthotics may occur.
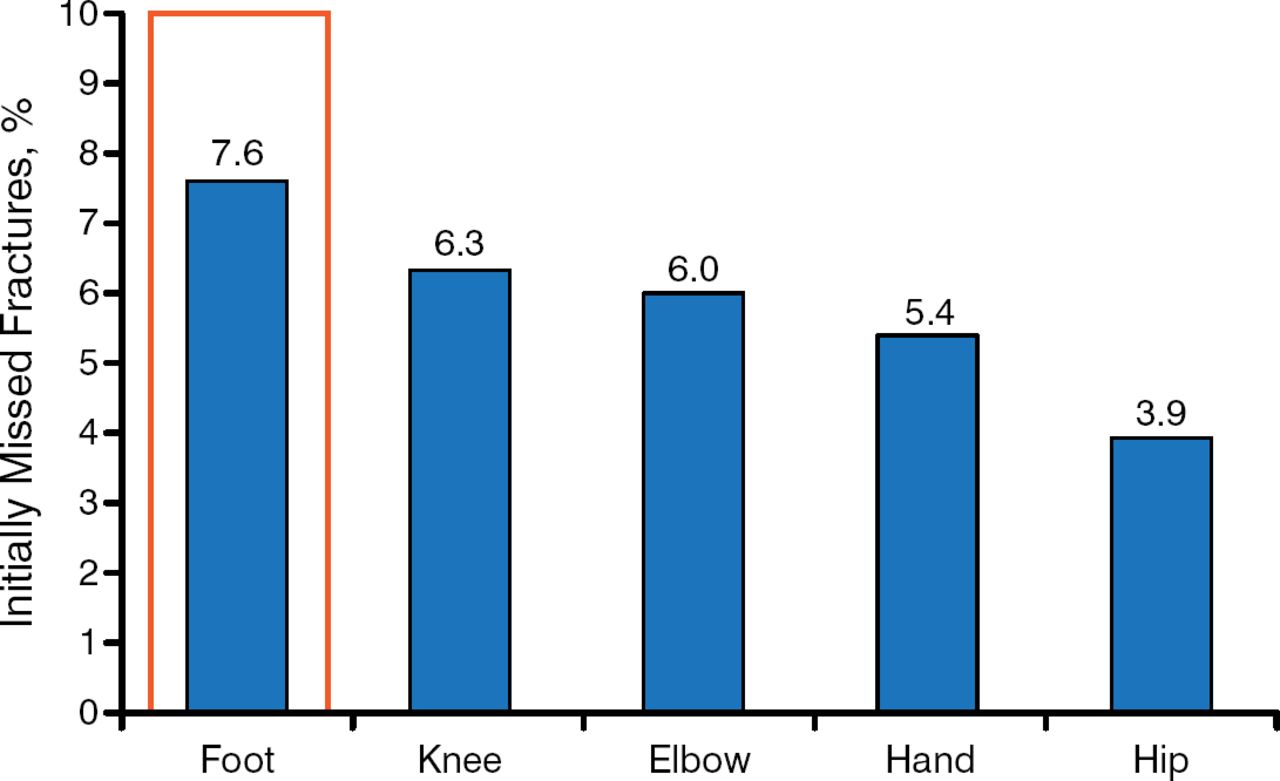
Paul T. Fortin, MD, William Beaumont Health System, Royal Oak, Michigan, USA, discussed how to manage missed midfoot injuries. The foot, the talus in particular, is the most common site of missed fractures, accounting for 7.6% of missed fractures on the first review (Figure 2) [Wei CJ et al. Acta Radiol. 2006].

Most Commonly Missed Fractures
Data source: Wei CJ et al. Acta Radiol. 2006.
Missed injuries of the foot are commonly associated with permanent physical impairment, often involve essential joints, and often present with limited salvage options. Missed injuries occur more often (10% more) in polytrauma patients who have poorer morbidity (degenerative joint disease, instability, neurogenic pain, and deformity) than those without foot injury [Richter M et al. Foot Ankle Int. 2001].
Greater awareness of midfoot mechanics, coupled motion, essential joints, and lateral tarsometatarsals can improve outcomes, according to Dr Fortin. Patterns of foot injury and radiographic clues can help identify occult injuries. Injuries should be evaluated as to pain source, associated deformity (location, magnitude, direction, and flexibility), equinus, soft-tissue status, possible bone loss, muscle imbalance, and comorbid factors (neuropathy, vasculopathy, and dystrophy).
Operative treatment of midfoot arthritis relieves pain only 60% of the time [Patel A et al. J Am Acad Orthop Surg. 2010]. Many patients have persistent gait disturbance and 10% require a second reconstruction. Acute treatment is better than delayed fusion. Salvage arthrodesis often is the only thing possible after delayed diagnosis. Treatment is based on restoring medial and lateral column relationship, preserving essential joint function, and addressing the associated deformity and soft tissue balance. Surgical approaches include Lazy S, double dorsal, Bohler/Hannover, and plantar techniques. Joint preservation can be attempted with a Chopart injury, but the outcome is poor with combined tarsometatarsal and Chopart fractures. Possible complications include metatarsalgia, lateral column pain, stress fracture, nonunion/malunion, and poor wound healing.
In summary, early recognition improves outcome and it is not always necessary to perform a fusion.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.