

Summary
There are multiple topical and systemic treatments, as well as phototherapy, available to effectively treat and reduce relapse of atopic dermatitis (AD). This article discusses adherence to treatment regimens in patients with AD, current topical treatment options, systemic treatment options, strategies to treat pruritus, as well as the role of phototherapy in AD.
- Skin Diseases
- Dermatology Treatments
- Dermatology
- Skin Diseases
- Dermatology Treatments
There are multiple topical and systemic treatments, as well as phototherapy, available to effectively treat and reduce relapse of atopic dermatitis (AD). Dusan Buchvald, MD, PhD, Comenius University, Bratislava, Slovakia, discussed adherence to treatment regimens in patients with AD. Nonadherence is defined as the underuse or overuse of medication, whether it be unintentional or deliberate. For example, some patients are physically unable to apply topical medication to certain affected body surfaces, such as the central back or feet [Ulff E et al. Br J Dermatol. 2007]. Up to 30% of prescriptions for topical treatments used in dermatology are never filled [Storm A et al. J Am Acad Dermatol. 2008], and only about 50% of patients who fill their prescriptions actually use their topical medication appropriately [Carroll CL et al. J Am Acad Dermatol. 2004]. In most cases, patients use an insufficient dose [Storm A et al. J Am Acad Dermatol. 2008].
Patients generally do not accurately self-assess their adherence to medication. In one study, patients recorded an adherence rate of 80% to 90% in a diary, whereas stealth monitoring found a decreasing rate of adherence to about 40% to 60% throughout 58 days [Carroll CL et al. J Am Acad Dermatol. 2004]. Patients indicated that they applied their therapy less often than prescribed due to lack of efficacy, staining of clothing and surfaces, time-consuming processes, fear of side effects, and cost. In contrast, overuse is due to a desire to clear lesions more rapidly, lack of efficacy, improved efficacy with increased use, and lack of side effects [Brown KK et al. J Am Acad Dermatol. 2006]. To improve adherence, Prof Buchvald suggested coming to a mutual agreement with the patient regarding the treatment plan.
Mette Deleuran, MD, DMSc, Aarhus University Hospital, Aarhus, Denmark, presented the current topical treatment options for AD. Filaggrin, an epidermal barrier protein, plays an important role in AD because loss-of-function genetic variants of filaggrin are associated with AD [Palmer CN et al. Nat Genet. 2006]. However, although all patients with AD have a skin barrier dysfunction, it is not always associated with a filaggrin mutation; instead, filaggrin deficiency can also be caused by inflammation, because cytokines like interleukin (IL)-4, IL-13, and IL-25, which are upregulated in AD, can downregulate the expression of filaggrin [Hvid M et al. J Invest Dermatol. 2011; Howell MD et al. J Allergy and Clinical Immunol. 2007]. Topical treatment with emollients and corticosteroids can substantially improve symptoms.
Infants who were at high risk of developing AD were treated daily with an emollient at a mean follow-up of 547 days. Only 3 of 20 patients developed AD [Simpson EL et al. J Am Acad Dermatol. 2010]. In another study, infants with AD were treated with moisturizer twice a day on uninvolved skin and topical corticosteroids as needed on involved skin during a period of 6 weeks. The study included a control group that was treated with only topical corticosteroids on involved skin. The amount of high-potency corticosteroid was reduced by 42% in the emollient-treated group compared to the control group [Grimalt R et al. Dermatology. 2007]. These studies suggest that use of emollient can reduce the need for corticosteroid treatment. Prof Deleuran recommends that emollients be applied every day, but toxic ingredients and allergens (eg, fragrance or peanut oil) should be avoided.
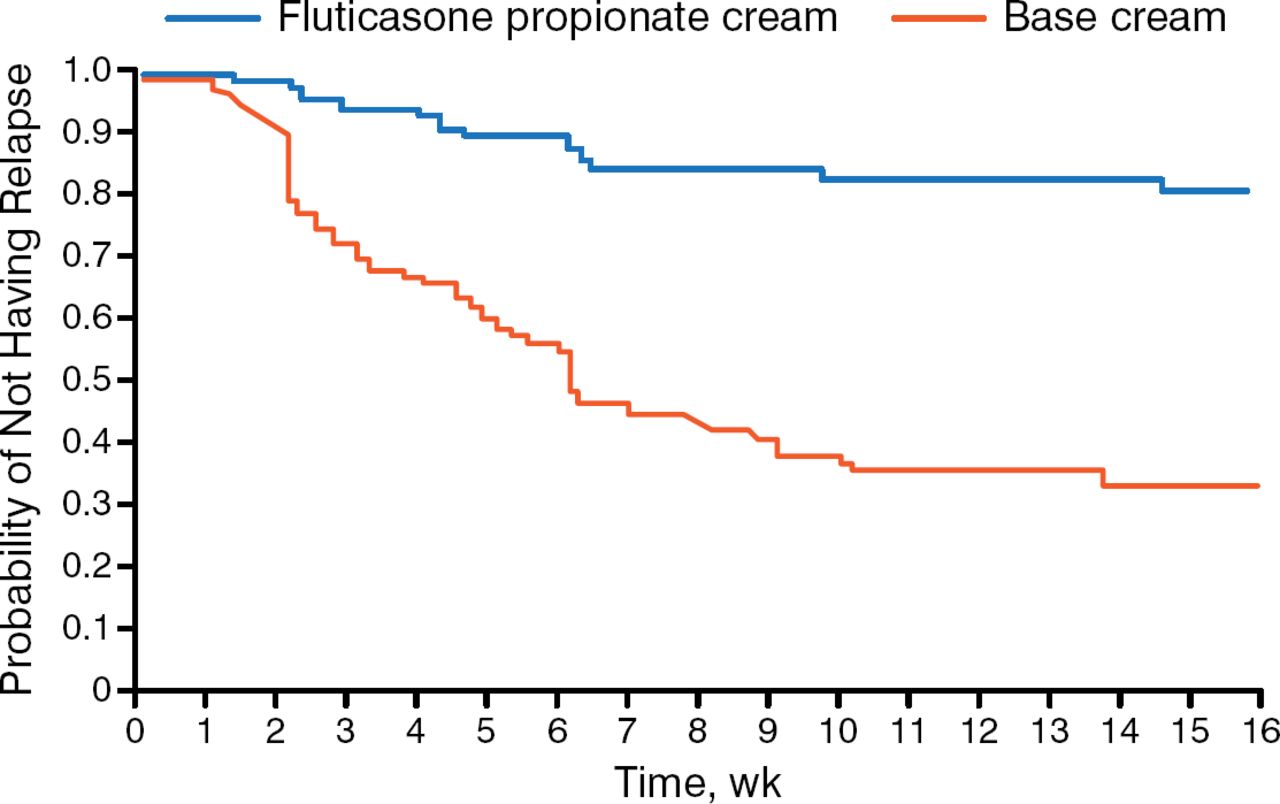
Topical corticosteroids are effective in treating AD lesions, although patients may fear potential side effects [Aubert-Wastiaux H et al. Br J Dermatol. 2011]. It can be helpful to define the use of the “fingertip” unit for patients, which dispenses about 0.5 g of ointment or cream and is enough to apply to the area of 2 adult handprints [Finlay AY. BMJ. 2012]. Proactive treatment is important in inducing and maintaining remission. Patients with AD who were treated with fluticasone propionate cream twice per week for a mean exposure of 337 days were 7.7 times less likely to experience a relapse compared with patients who received placebo (Figure 1) [Hanifin J et al. Br J Dermatol. 2002]. In another study, proactive treatment with tacrolimus resulted in a prolonged median time to the first flare and fewer flares compared with patients who received reactive treatment [Wollenberg A et al. Allergy. 2008].

Effect of Proactive Treatment on Atopic Dermatitis Relapse
Reproduced from BMJ, Berth-Jones J et al, Twice weekly fluticasone propionate added to emollient maintenance treatment to reduce risk of relapse in atopic dermatitis: randomized, double blind, parallel group study. 2003;326:1367. With permission from BMJ Publishing Group Ltd.
Systemic Therapy of Atopic Dermatitis
Andreas Wollenberg, MD, Ludwig-Maximilian University, Munich, Germany, discussed systemic treatment options for AD, including oral corticosteroids and cyclosporine (CyA).
Multiple phase 2 trials are underway evaluating monoclonal antibodies that target IL-31, IL-31 receptor, IL-22, IL-12/IL-23, and thymic stromal lymphopoietin, as well as a CRTH2 inhibitor. In addition, an IL-4 receptor monoclonal antibody is being evaluated in a phase 3 trial [NCT02260986]. For example, treatment with the monoclonal antibody targeting the IL-31 receptor, CIM331, and the IL-4/IL-13 monoclonal antibody, dupilumab, resulted in an improvement in AD as measured by the Eczema Area and Severity Index (EASI) and pruritus compared with baseline [Beck LA et al. N Engl J Med. 2014]. In another study, dupilumab plus topical corticosteroid treatment demonstrated improvement in the EASI-50 by day 15 compared with placebo plus corticosteroid [NCT01639040].
Lukasz Matusiak, MD, PhD, Wroclaw Medical University, Wroclaw, Poland, presented on the behalf of Jacek C. Szepietowski, MD, PhD, Wroclaw Medical University, and described strategies to treat pruritus in patients with AD. In AD, pruritus can be quite severe, with patients reporting the intensity of the itch to be greater than that of psoriasis and chronic urticaria [Darsow U et al. Itch: Mechanisms and Treatment. 2014; Yosipovitch G et al. Int J Dermatol. 2002]. Pruritus causes difficulty with falling asleep and increases awakenings in both adults and children [Yosipovitch et al. Int J Dermatol. 2002]. In addition, pruritus intensity has been associated with self-assessed stress and depression [Chrostowska-Plak D et al. J Eur Acad Dermatol Venereol. 2013].
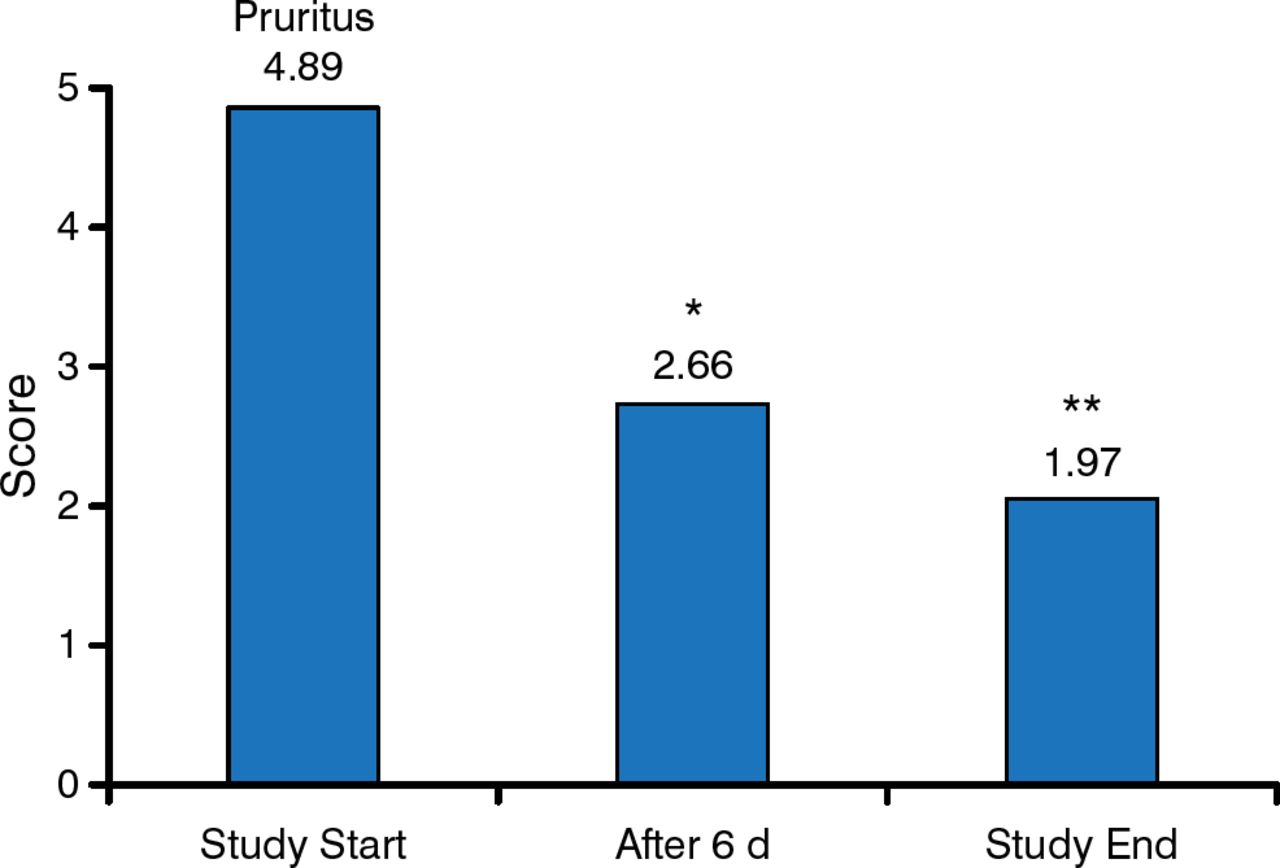
Risk factors that can increase pruritus in AD include irritants, allergens, skin dryness, physical effort, sweating, hot baths, and stress. Treatment of pruritus with antihistamines has largely shown little to no improvement, except for treatment with fexofenadine; however, sedating antihistamines may be useful during nighttime to improve sleep [Weisshaar E et al. Acta Derm Venereol. 2012]. Emollients may also improve pruritus symptoms. A study in pediatric patients with AD who received 0.1% methylprednisolone once daily with or without a twice-daily emollient demonstrated a significant improvement in EASI (P = .01) and itching intensity [Szczepanowska J et al. Pediatr Allergy Immunol. 2008]. Furthermore, treatment with an emollient containing an endocannabinoid receptor agonist resulted in a significant decrease in pruritus (P < .001) and loss of sleep (P < .001) at 6 days and study end (Figure 2) [Eberlein B et al. J Eur Acad Dermatol Venereol. 2008]. Calcineurin inhibitors, such as tacrolimus, have been shown to decrease itch by inhibiting immunoglobulin E mast cell degranulation and decreased sensitivity of VR1 receptors [Ständer S, Luger TA. Hautarzt. 2003].

Emollient-Containing Endocannabinoid Receptor Agonist Improves Itch
*P < .001 vs study start.
**P < .001 vs day 6.
Reprinted from Eberlein B et al. Adjuvant treatment of atopic eczema: assessment of an emollient containing N-palmitoylethanolamine (ATOPA study). J Eur Acad Dermatol Venereol. 2008;22:73–82. With permission from European Academy of Dermatology and Venereology.
Martin Röcken, MD, Eberhard Karls University Tübingen, Tübingen, Germany, outlined the role of phototherapy in AD. Prof Röcken noted that phototherapy includes the use of broad-spectrum ultra violet B (UVB) light from 280 to 320 nm, small-spectrum UVB at 311 nm, psoralen ultraviolet A (PUVA) at 320 to 400 nm, and medium-dose UVA1 at 340 to 400 nm. Phototherapy is useful in patients with AD because it improves 3 of the major underlying mechanisms, which are barrier defects, bacterial superinfection, and T cell-mediated inflammation.
In normal human keratinocytes, ultraviolet exposure resulted in the upregulation of antimicrobial peptides, including human β-defensin-2, human β-defensin-3, ribonuclease 7, and psoriasin (S100A7) [Glaeser R et al. J Allergy Clin Immunol. 2009]. In addition, UVB exposure of human skin grafted to nude mice causes the barrier protein filaggrin to normalize [Del Bino S et al. Br J Dermatol. 2004].
Prof Röcken also noted that small-spectrum UVB is effective for all types of AD and that dosing begins at 60% of the minimal erythema dose. Systemic PUVA therapy is effective for severe prurigo, a finding in some cases of AD, and is initially dosed at 75% of the minimal phototoxic dose for 4 days, followed by 2 times a week for 4 weeks and then once weekly. A 20-minute warm water bath with a methoxsalen solution can be added prior to PUVA therapy. UVA1 therapy is effective for acute AD, and although the device is expensive, it does not cause sunburn because all of the UVB rays are filtered out. There is, however, a higher risk of phototoxicity related to drug- and food-induced sensitivity. Although rarely used, phototherapy can be combined with systemic treatments for AD, including methotrexate and potentially azathioprine; however, phototherapy cannot be combined with CyA.
In conclusion, there are multiple therapeutic options for the treatment of AD. To reduce relapse, emollients should be used daily. To treat lesions, however, systemic therapies and phototherapy are effective when patients adhere to their regimen. In addition, it is important to consider treating pruritus, because pruritus can be debilitating.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.