

Summary
During the Emery A. Rovenstine Memorial Lecture, the state of health care in the United States was discussed. The Lecture stressed that health care is changing at an enormous rate and it is imperative for anesthesiologists to change and adapt to this new dynamic environment and or risk losing their contracts or jobs to competitors.
- Anesthesiology
- Anesthesiology
Karen B. Domino, MD, MPH, University of Washington, Seattle, Washington, USA, presented the Emery A. Rovenstine Memorial Lecture, during which she shared her views on the state of health care in the United States based on insight garnered as a Robert Wood Johnson Foundation health policy fellow working with the House Committee on Ways and Means.
Dr Domino believes that health care is changing at an enormous rate and it is imperative for anesthesiologists to change and adapt to this new dynamic environment and or risk losing their contracts or jobs to competitors. Independence is being eroded as more and more physicians, surgeons, and specialists are being employed by large health care systems. During her fellowship tenure, Dr Domino saw a tendency for both government parties to “kick the can” from one desk to the next, leaving many problems unsolved in the face of outside powerful forces pushing for health care change. She suggested that economics, not Obamacare, is the main driving force and that it is not the government's job to tame these forces—health care workers should be leading the way for change.
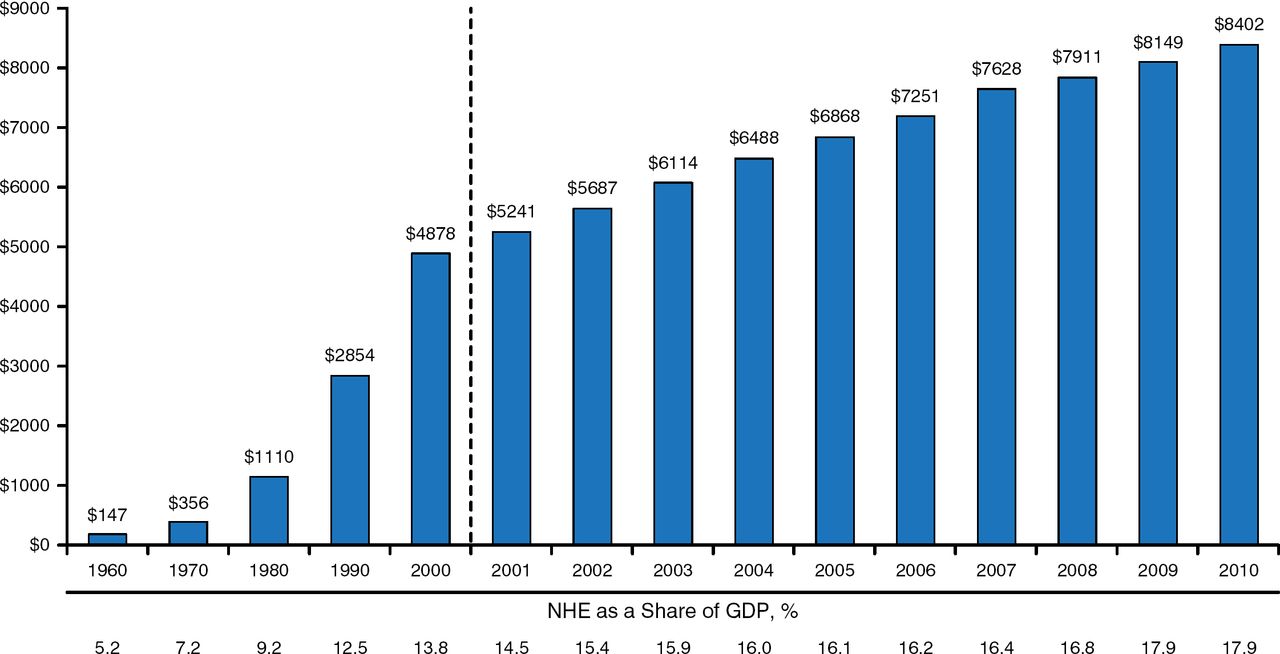
Despite the passage of the Patient Protection and Affordable Care Act, the cost of US health care continues to increase, jumping from approximately $4900 per capita per year in 2000 to nearly $8400 in 2010. Health care costs are 8 times what they were in 1980 and US spending on health care is 2.5 times that of any other developing nation (Figure 1), accounting for 17.7% of the 2011 gross domestic product (GDP) [US Centers for Medicare and Medicaid Services Office of the Actuary, National Statistics Group. 2011].

Increasing Health Expenditures per Capita: 1960–2010
GDP, gross domestic product; NHE, national health care expenditure.
Reproduced from Centers for Medicare & Medicaid Services. CMS Office of the Actuary, National Statistics Group 2011. Available at http://www.cms.hhs.gov/NationalHealthExpendData/. Accessed November 7, 2014.
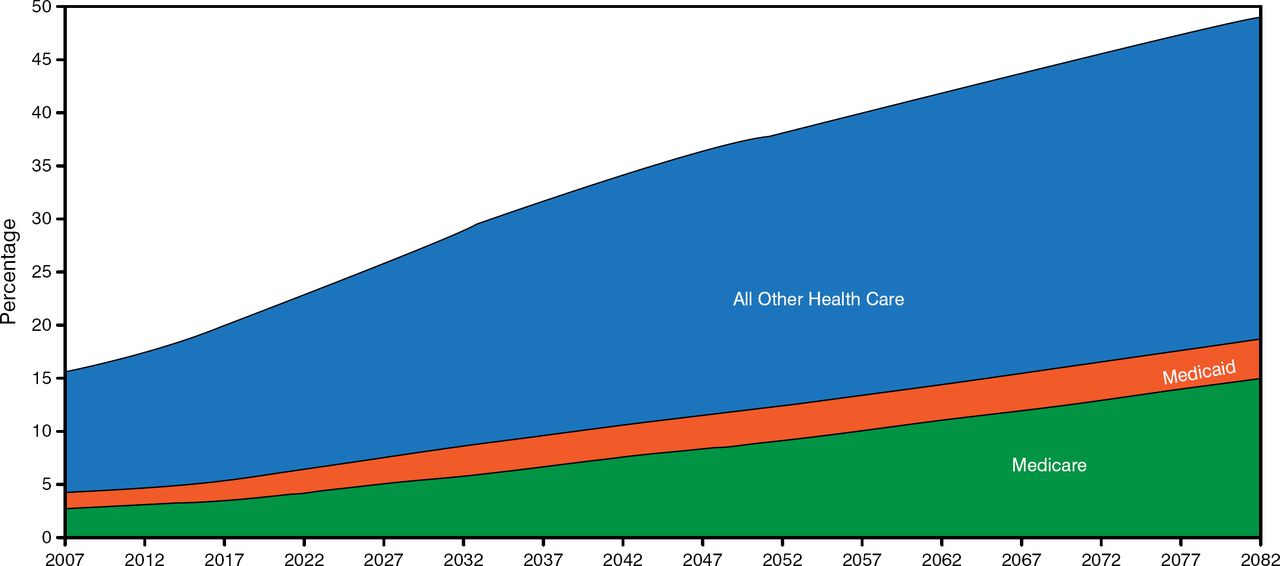
As baby boomers reach the retirement age, health care costs will continue to rise and will soon become unsustainable. According to the US Congressional Budget Office, projections for health care spending will double by 2035 to 31% of GDP, reaching 49% by 2082, at which point it will overtake a large proportion of the funds needed in other areas (Figure 2) [Congressional Budget Office Report. 2007]. This is the prime reason for the need to change our health care system.

Projected Spending on Health Care as a Percentage of the Gross Domestic Product
Reprinted from Congress of the United States. The Long–Term Outlook for Health Care Spending: Sources of Growth in Projected Federal Spending on Medicare and Medicaid. Issued November 2007. Congressional Budget Office. Available at http://www.cbo.gov/sites/default/files/11-13-lt-health.pdf. Accessed 11/6/2014.
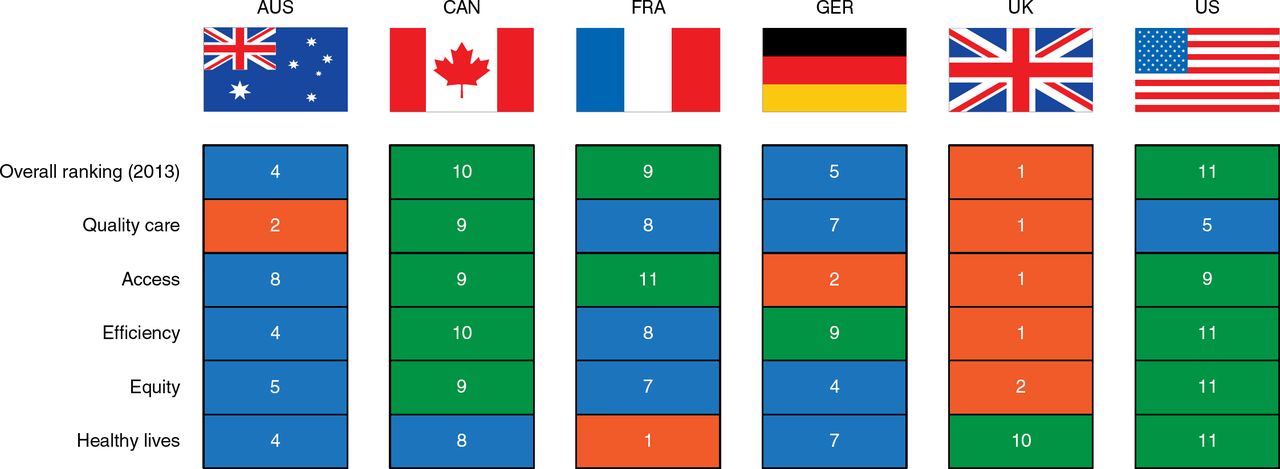
Despite the high expenditures on health care, the care we receive is of poor quality. Life expectancy is the United States is lower than in our peer nations (27th out of 34 nations), according to a 2013 report published in JAMA [US Burden of Disease Collaborators. JAMA. 2013]. In the 2014 Commonwealth Fund Update, US health care ranked last in almost every category among developed nations (Figure 3) [The Commonwealth Fund Update. 2014].

Ranking of US Health Care With Other Developed Nations
Adapted from Davis K et al. 2014. Mirror, Mirror on the Wall. The Commonwealth Fund 2014 Update. With Permission from The Commonwealth Fund.
Payers (consumers, businesses, and government) want a value–driven system that improves quality, instead of the current system, which is volume driven and in which physicians and hospitals are paid for providing more and more services and the fee–for–service system pays even more if complications occur.
Innovations that bring US health care costs into a sustainable range are needed for both public and private payers. Consumers need to have more say in their care. Payers look more critically at quality and value when they directly pay for what they are buying with money out of their own pockets. Reference pricing is needed to establish a fair price for an imaging test or a surgical procedure. Prices for procedures can currently vary by thousands of dollars depending on where the procedure is performed and who performs it. Transparency in costs as well as in quality of care is needed to enable value comparison. Value–based purchasing would enable a company to contract with a health care system that would allow an employee to travel to an alternative medical center where the procedure is performed for a set price.
The opportunity to cut costs through less waste is immense. It is estimated that 6 categories of waste (overtreatment, failures of care coordination, failures in execution of care processes, administrative complexity, pricing failures, and fraud and abuse) account for 34% of health care spending [Berwick DM, Hackbarth AD. JAMA. 2012].
“Now is not the time for business as usual,” said Dr Domino. Now is the time for new leadership. Physicians need to become stewards of our finite health care resources. Physicians near retirement should become champions of initiatives that their hospitals consider important. Mid–career anesthesiologists need to rethink how to standardize systems of care to reduce variability, errors, and costs. “We are in a new age of anesthesia care,“ she said, where effective leadership, blended care teams with fewer anesthesiologists in order to eliminate or reduce hospital subsidies, and the routine provision of quality and performance data to hospital administrations are needed.
The focus should shift toward creating standard–guided systems of care that rate how well goals are being met, redesigning surgical decision making for high–risk patients that takes into account what the patient or family would like, renewing the focus on teaching the management of patients during the perioperative period, and training a new generation of anesthesiologists. Young anesthesiologists need to learn how to lead teams, manage operating rooms, and manage change. Fellowship training should cover internal medicine, surgical outcomes, perioperative care, care transitions, and long–term recovery. To prepare for this transformation, today's anesthesiologists will need to understand informatics, implementation of science, systems management, and health policy.
Dr Domino has returned to her roots in Seattle, and she pointed out the lessons she learned concerning the changes overwhelming the health care system:
-
▪ Like an automobile accident, you could see it happening, but you couldn't stop it.
-
▪ We should have been more focused on quality and performance.
-
▪ Hospitals expected more leadership in preoperative clinic and operating room management.
-
▪ Younger colleagues are more attuned to changes needed; listen to them.
-
▪ No group is too big to be replaced.
Dr Domino concluded that “The clock is ticking. The time to act is now.”
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.