

Summary
This article presents data from a study that was conducted to assess the long-term results of primary anterior cruciate ligament (ACL) reconstructions using either allograft or autograft. The results showed that, in a young, athletic population, reconstructed ACLs failed 3 times as often with allografts compared with autografts.
- Orthopaedics Clinical Trials
- Hip & Knee Conditions
- Orthopaedic Procedures
- Sports Medicine
- Orthopaedics
- Orthopaedics Clinical Trials
- Hip & Knee Conditions
- Orthopaedic Procedures
- Sports Medicine
Craig R. Bottoni, MD, Tripler Army Medical Center, Honolulu, Hawaii, USA, presented data from a study that was conducted to assess the long-term results of primary anterior cruciate ligament (ACL) reconstructions using either allograft or autograft. The results showed that, in a young, athletic population, reconstructed ACLs failed 3 times as often with allografts compared with autografts.
ACL reconstructions are becoming increasingly common, and with > 250,000 tears occurring each year in the United States, resulting in > 100,000 reconstructions, the use of allografts is also becoming more common. With this in mind, Dr. Bottoni and colleagues conducted a prospective, randomized controlled study to compare the long-term clinical and subjective outcomes after 100 primary ACL reconstructions in 99 patients with a symptomatic ACL-deficient knee who received either hamstring autograft tissue (n = 50; mean age, 28.9 years) or tibialis posterior tendon allografts (n = 50; mean age, 29.2 years).
Participants were predominantly active-duty military personnel. All allografts were from a singular American Association of Tissue Banks—approved tissue bank, and they were aseptically processed and fresh frozen without terminal irradiation. Graft fixation was the same in all cases, and all patients followed the same rehabilitation protocol, using physical therapists who were blinded to their patients' surgical procedure. Patients underwent preoperative and postoperative assessments of graft integrity, knee stability, and functional status, and they also completed telephone- and Internet-based questionnaires.
Exclusion criteria included patients younger than 18 years old, as well as those who had multiligamentous injury or had undergone previous knee ligament surgery. The primary outcomes were graft integrity, subjective knee stability, and functional status.
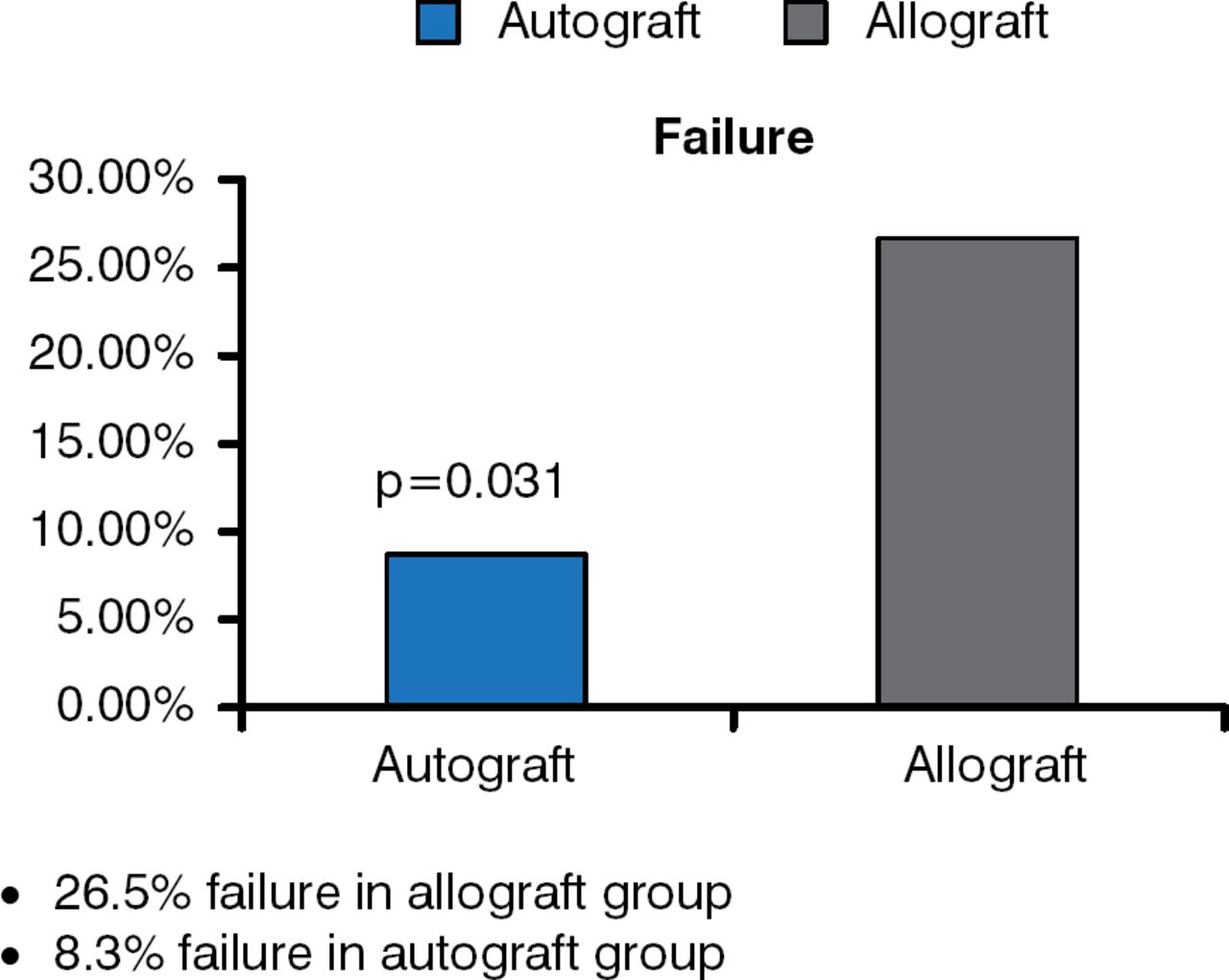
After a minimum of 10 years of follow-up, 2 patients died, and 1 was lost to follow-up. In the population that remained for analyses, however, more than 80% of all grafts remained intact and had maintained stability. Autografts had a failure rate of 8.3%, however, compared with 26.5% for allografts (p = .031; Figure 1). Dr. Bottoni pointed out that although these findings are in contrast to previous reports of similar failure rates of autografts and allografts in a young, athletic population of patients, those data did not derive from randomized controlled trials.

Comparison of Failure Rate Using Allograft Versus Autograft
Reproduced with permission from CR Bottoni, MD.
In the remaining patients whose graft was intact, there was no difference in the mean Single Assessment Numeric Evaluation, Tegner, or International Knee Documentation Committee scores.
Dr. Bottoni acknowledged that some limitations of this study included the subjective assessment of graft stability as well as the fact that the study involved only the tibialis posterior type of allograft. Consequently, the results can be applied to only this type of allograft and cannot be extrapolated to other types of allografts. It is therefore possible that other types, particularly those with bone, such as the bone—patellar tendon—bone or Achilles grafts, may have resulted in different outcomes, concluded Dr. Bottoni.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.