

Summary
Fernando Brandao, MD, University of São Paulo, São Paulo, Brazil, described a prospective randomized trial comparing midshaft clavicular fractures treated with reconstruction plate fixation or elastic stable intramedullary nailing (ESIN).
Fernando Brandao, MD, University of São Paulo, São Paulo, Brazil, described a prospective randomized trial comparing midshaft clavicular fractures treated with reconstruction plate fixation or elastic stable intramedullary nailing (ESIN).
Midshaft clavicular fractures make up 80% of all clavicular fractures. Treatment seeks to reduce nonunion of the bone, speed recovery, and produce better functional outcome [Smekal V et al. J Orthop Trauma. 2009; Canadian Orthopaedic Trauma Society. J Bone Joint Surg Am. 2007]. The conventional treatment involves plate fixation, including reconstruction plates that can be molded to the desired clavicle shape. ESIN, which uses titanium elastic nails, is a more recent development [Jubel A et al. Kongressband Dtsch Ges Chir Kongr. 2002]. The techniques have been compared in only a few studies, which were mainly retrospective [Chen YF et al. J Shoulder Elbow Surg. 2012; Tarng YW et al. J Shoulder Elbow Surg. 2012; Assobhi JE. J Orthop Traumatol. 2011].
The present single-center clinical trial compared the 2 approaches in terms of the Disabilities of the Arm, Shoulder, and Hand (DASH) score at 6 months postoperatively. Secondary outcomes were DASH score at 12 months, Constant-Murley shoulder outcome (pain and function) score at 6 and 12 months, time to bone union, clavicle shortening, visual analog scale assessment of pain, and complications.
Fifty-nine patients who were enrolled from May 2010 to January 2013 were randomly allocated to receive plate fixation (n = 33) or ESIN (n = 26): 29 and 25, respectively, completed the follow-up. The 59 patients were 16 to 65 years of age (mean 29.9 ± 11.1 years). The majority (n = 47) were male. Shoulder injuries were the result of motorcycle accidents in 54% of patients and falls in 20%. The AO/OTA classification of fractures and dislocations was B1 (39%), B2 (41%), and B3 (20%).
The mean DASH scores at 6 months were 9.9 and 8.5 in the plate and ESIN groups, respectively (P = .329). The 12-month DASH scores were similar (P = .496). Constant-Murley scores for both groups at 6 and 12 months were virtually identical (P = .999 and P = .937). No significant differences were evident in time to union (16.8 weeks in the plate group and 15.9 weeks in the ESIN group; P = .352) and visual analog scale rating of pain (P = .673).
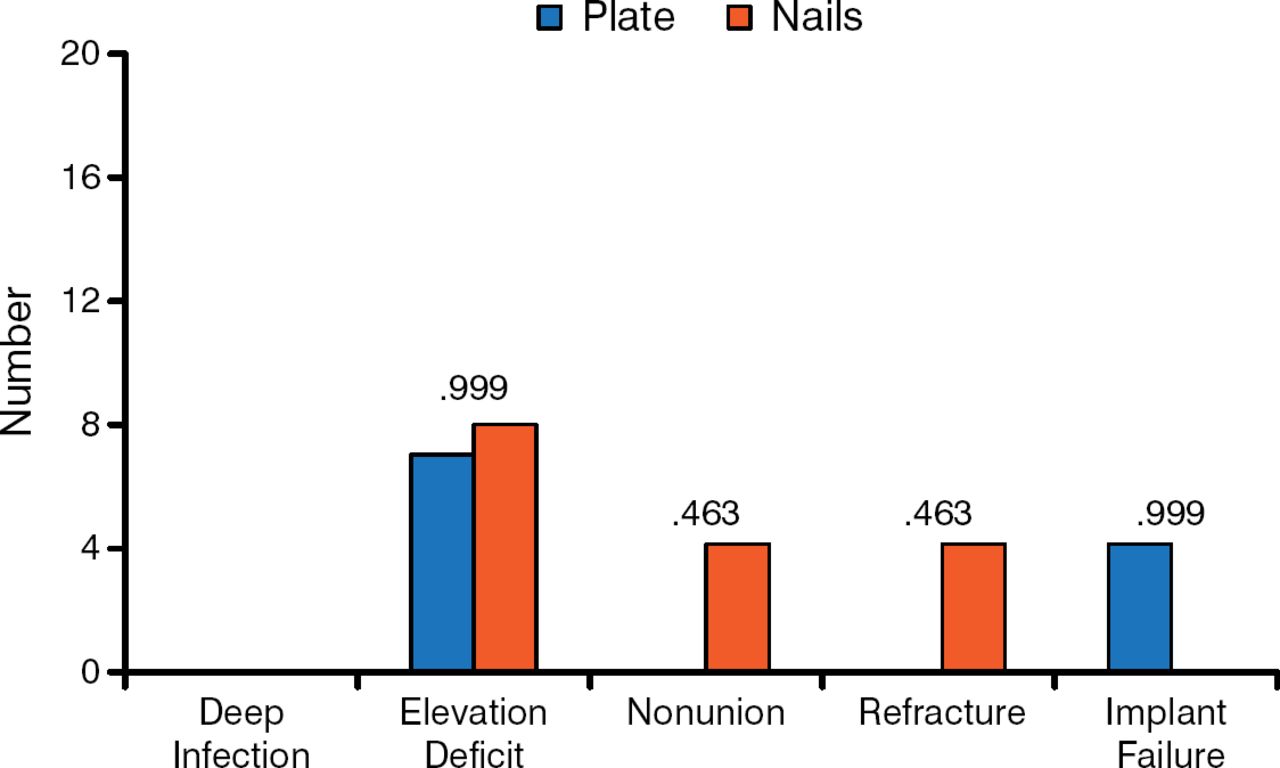
Residual shortening was significantly greater in the plate group (P = .032). However, the actual value of 0.4 cm was not clinically relevant. Hardware-related pain was greater in the ESIN group (n = 10) than in the plate group (n = 4; P = .035). The rate of implant bending and subsequent shortening of the clavicle was significantly greater in the plate group (n = 11) as compared with 1 patient in the ESIN group (P = .003). Comparison of the DASH and Constant-Murley scores at 6 and 12 months between patients with bent and nonbent reconstruction plate implants did not reveal significant differences. However, time to union was significantly longer in patients with a bent implant (P = .044). Major complications occurred at similar frequency in both groups (Figure 1).

Major Complications in the Plate and Elastic Stable Intramedullary Nailing Groups
Reproduced with permission from F Brandao, MD.
The data indicate the similar efficacy and safety of the methods in promoting fracture healing. Reconstruction plates can bend owing to reduced stiffness and thus can be less reliable in maintaining alignment of the healing fracture. ESIN can produce more discomfort to the point of implant removal.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.