

Summary
A secondary prespecified substudy analysis of the Administration of Ticagrelor in the Cath Lab or in the Ambulance for New ST Elevation Myocardial Infarction to Open the Coronary Artery [ATLANTIC; NCT01347580] assessed whether prehospital administration of the direct-acting platelet P2Y12 receptor antagonist ticagrelor can improve coronary reperfusion and clinical outcomes in patients with STEMI. The results are discussed in this article
- Cardiology Clinical Trials
- Myocardial Infarction
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Myocardial Infarction
- Cardiology
- Interventional Techniques & Devices
For patients with ongoing STEMI, prehospital administration of ticagrelor approximately 45 to 60 minutes prior to undergoing percutaneous coronary intervention (PCI) improves ST elevation segment resolution after PCI without increasing bleeding.
Arnoud W. J. van't Hof, MD, Isala Klinieken, Zwolle, The Netherlands, presented the results of a secondary prespecified substudy analysis of the Administration of Ticagrelor in the Cath Lab or in the Ambulance for New ST Elevation Myocardial Infarction to Open the Coronary Artery [ATLANTIC; NCT01347580], an international multicenter double-blind study to assess whether prehospital administration of the direct-acting platelet P2Y12 receptor antagonist ticagrelor can improve coronary reperfusion and clinical outcomes in patients with STEMI.
ATLANTIC randomized 1862 patients with STEMI who were < 6 hours from symptom onset to 1 of 2 ticagrelor administration groups: prehospital (in the ambulance; n = 909) or in hospital (in the catheterization laboratory; n = 953) [Montalescot G et al. N Engl J Med. 2014]. The average age of the patients was 61 years; approximately 19% had a body mass index of ≥ 30 kg/m2; nearly 13% had diabetes; and most were men (about 80% in each treatment group).
The prespecified substudy, called PRIVATE-ATLANTIC, focused on the effect of early ticagrelor administration on ST elevation resolution after PCI in this same cohort of patients. PRIVATE-ATLANTIC found a trend toward ST segment resolution in patients in the prehospital group as compared with the in-hospital group (42.5% vs 47.5%; P = .055). However, significantly more patients in the prehospital group had a degree of ST segment elevation resolution as compared with the in-hospital group (median, 75.0% vs 71.4%; P = .049).
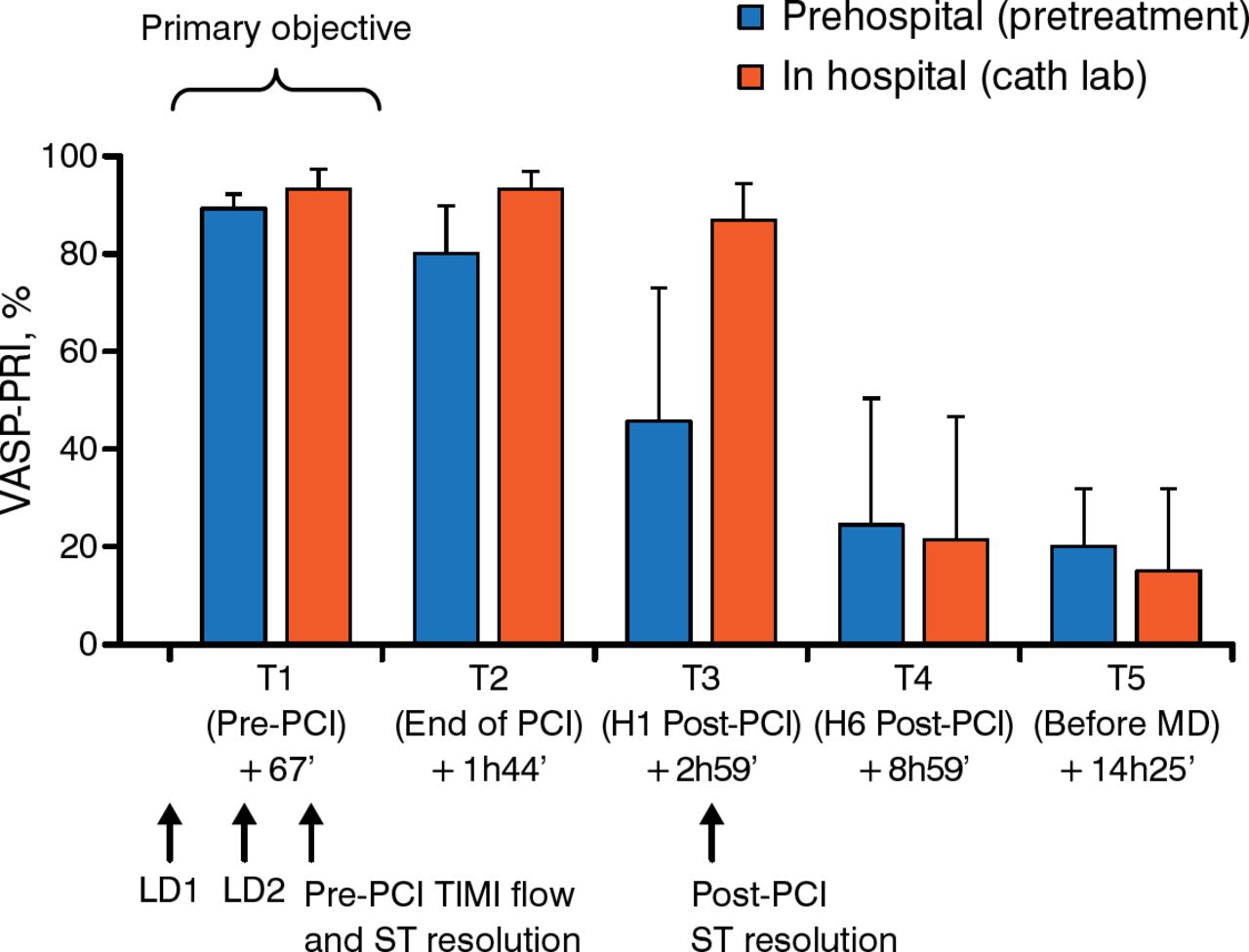
Regarding the effect of early ticagrelor on platelet aggregation inhibition, there was no significant difference between the prehospital and in-hospital groups before and after PCI (Figure 1). Prof van't Hof emphasized that most of platelet inhibition from ticagrelor is seen after PCI.

Effect of Ticagrelor on Platelet Inhibition
All comparisons (prehospital vs in-hospital), nonsignificant.
Cath lab, catheter laboratory; H/h, hour; LD, loading dose; MD, maintenance dose; PCI, percutaneous coronary intervention; T, time; VASP-PRI, vasodilator-stimulated phosphoprotein-platelet reactivity index.
Reproduced with permission from AWF van't Hof, MD.
The study also showed the importance of complete ST segment elevation resolution on major adverse cardiac events (MACEs). The incidence of MACEs and all-cause death up to 30 days after PCI was higher in patients with incomplete resolution vs those with complete resolution (5.9% vs 2.0% and 2.6% vs 1.1%, respectively). In addition, more patients with incomplete resolution had definite stent thrombosis up to 30 days after PCI as compared with patients with complete resolution (1.4% vs 0.3%).
The impact of complete vs incomplete ST segment elevation resolution after PCI on 30-day clinical end points is shown in TABLE 1, including a significant increase in the odds of all-cause death in patients with incomplete ST segment elevation resolution.
Effect of ST Segment Elevation Resolution After PCI on Clinical Outcomes
According to Prof van't Hof, this supports the validity of using complete ST-segment elevation resolution as a surrogate marker for CV clinical outcomes in patients with STEMI.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.