

Summary
Although the diagnosis of transient ischemic attack (TIA) can be challenging, identifying potential TIAs is imperative for urgent evaluation and treatment for preventing stroke. This article discusses the management of patients with TIA with particular focus on assessment of stroke risk.
- Episodic & Paroxysmal Disorders
- Cerebrovascular Disease
- Critical Care
- Prevention & Screening
- Episodic & Paroxysmal Disorders
- Cerebrovascular Disease
- Critical Care
- Prevention & Screening
- Emergency Medicine
Although the diagnosis of transient ischemic attack (TIA) can be challenging, identifying potential TIAs is imperative for urgent evaluation and treatment for preventing stroke [Castle J et al. Stroke. 2010]. Andrew W. Asimos, MD, Carolinas Medical Center, Charlotte, North Carolina, USA, discussed the management of patients with TIA with particular focus on assessment of stroke risk.
According to Dr Asimos, TIA has been defined traditionally as a sudden, focal neurologic deficit that lasts for < 24 hours. In 2009, however, the American Heart Association and American Stroke Association's scientific statement defined TIA as a transient event of neurologic dysfunction resulting from focal brain, spinal cord, or retinal ischemia without the presence of acute infarction [Easton JD et al. Stroke. 2009]. The duration of TIA symptoms is associated with positive diffusion-weighted imaging (DWI), with DWI positivity in about 30% of patients with symptoms lasting up to 6 hours and DWI positivity in about 50% of patients with symptoms lasting from 6 to 24 hours.
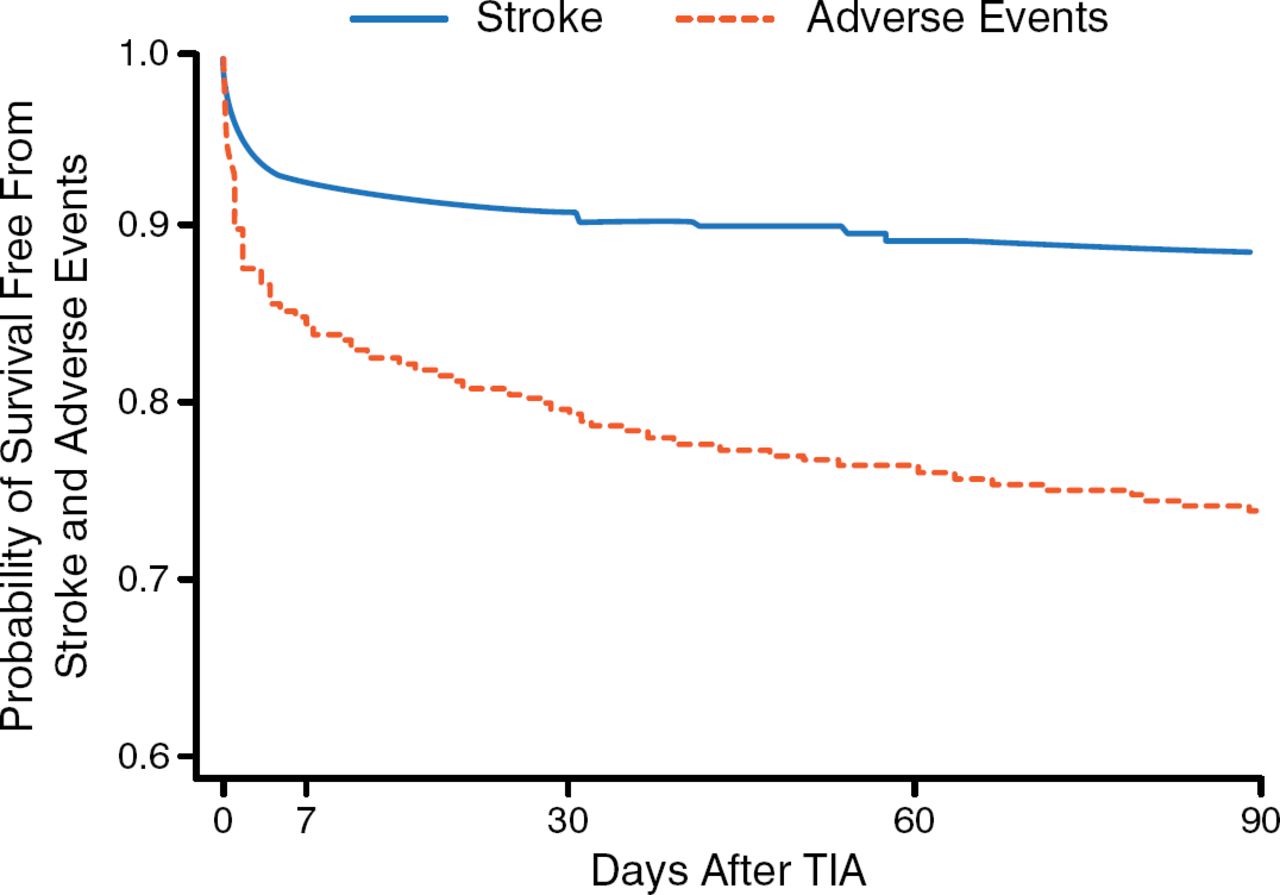
Fifteen years ago, about 10% of patients who experienced a TIA developed a stroke within 90 days, but more recent studies have found 90-day subsequent stroke rates of 2% to 3% [Lavallée PC et al. Lancet Neurol. 2007; Rothwell PM et al. Lancet. 2007; Perry JJ et al. CMAJ 2011]. This decrease in stroke rates is most likely attributable to more immediate investigation and aggressive management during the past 15 years. Nonetheless, the greatest risk period for early recurrent events remains the first few days after the index TIA (Figure 1) [Johnston SC et al. JAMA. 2000]. Although risk stratification tools are appealing to help identify patients who are at the greatest risk of early stroke, none of the tools is sufficiently discerning to determine early risk, because high stroke rates have been found in patients predicted to be low risk [Lemmens R et al. Stroke. 2013].

Risk of Stroke After TIA
TIA, transient ischemic attack.
Adapted from Johnston SC et al. Short-term Prognosis After Emergency Department Diagnosis of TIA. JAMA. 2000;284:2901–2906. Copyright © (2000) American Medical Association. All rights reserved
For example, 1 study found that a low ABCD2 score (≤ 3) has only an 87.3% (95% CI, 83.1% to 90.6%) sensitivity of identifying patients who have a low risk of developing ischemic stroke within 7 days from the TIA [Asimos AW et al. Ann Emerg Med. 2010], whereas another study found the ABCD2 score to be inaccurate at any cutpoint as a predictor of imminent stroke (Table 1) [Perry JJ et al. CMAJ. 2011]. One reason for this may be changes in diagnostic definitions and interventions, which may alter performance of the scores.
Sensitivity of ABCD2 Risk Score at 7 Days
A more promising TIA risk score in development is the Canadian TIA Score, which encompasses a range of clinical findings (eg, duration of symptoms, antiplatelet therapy, and triage diastolic blood pressure), as well as investigations in the emergency department (eg, atrial fibrillation on echocardiogram, platelet count, and glucose level) [Perry JJ et al. Stroke. 2014].
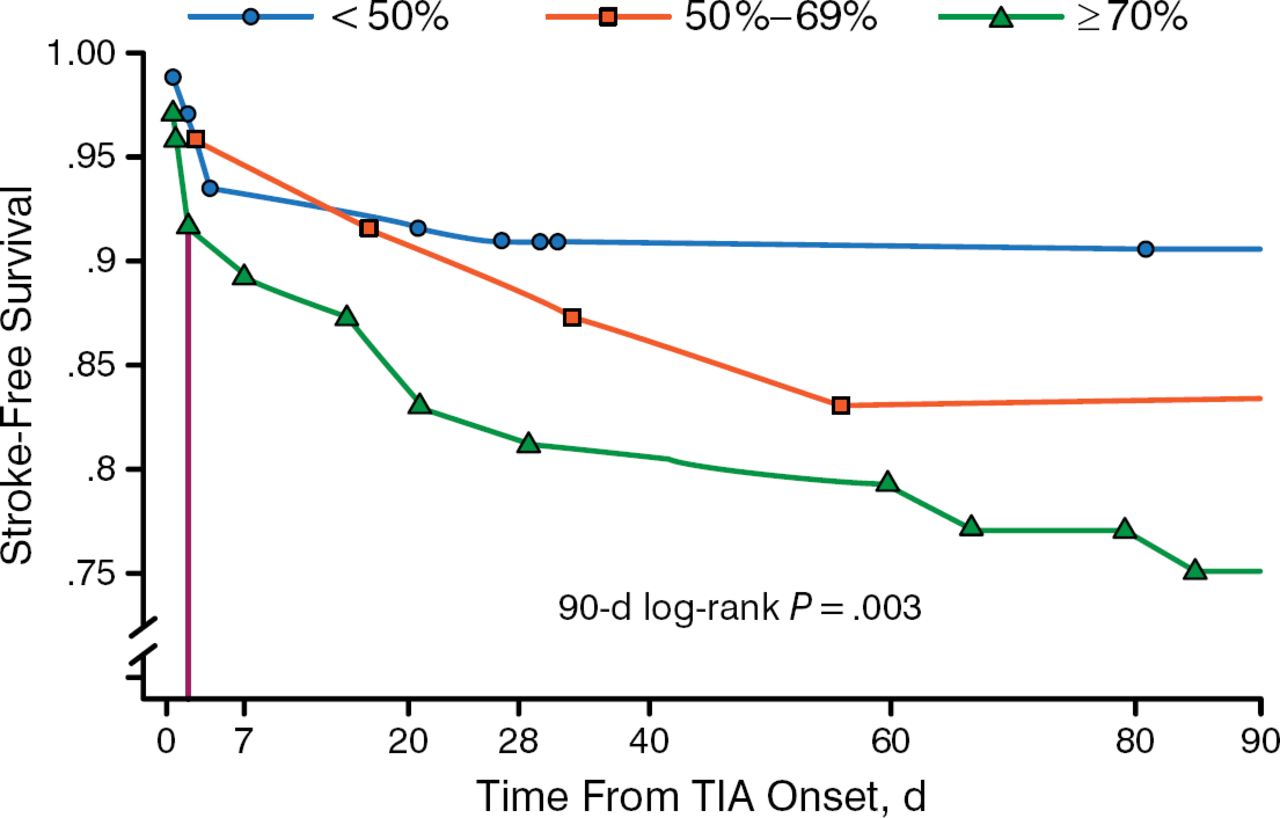
TIA patients with angiographic evidence of stenosis are at an increased risk of experiencing stroke. Furthermore, the location of disease influences the extent of the risk. In the Oxford Vascular Study [Neurology. 2004], the greatest risk of stroke (almost 20%) was associated with large-artery atherosclerosis and the lowest risk of stroke (< 5%) was associated with small-vessel disease. In another study, patients with ≥ 70% carotid artery stenosis were significantly more likely to experience stroke at 90 days (Figure 2) [Sheehan OC et al. Stroke. 2010]. Dr Asimos pointed out that in patients with ≥ 70% carotid artery stenosis, increased risk of stroke occurred early, beginning within 7 days after TIA.

Effect of Carotid Artery Stenosis on Risk of Stroke
TIA, transient ischemic attack.
Adapted from Sheehan OC et al. Population-Based Study of ABCD2 Score, Carotid Stenosis, and Atrial Fibrillation for Early Stroke Prediction After Transient Ischemic Attack. Stroke. 2010;41:844–850. With permission from American Heart Association.
Recent studies have evaluated the impact of TIA management on subsequent outcomes. The EXPRESS [Rothwell PM et al. Lancet. 2007] and SOS-TIA [Lavallee PC et al. Lancet. 2007] studies evaluated patients with TIA in a dedicated outpatient unit, which resulted in fewer than expected subsequent strokes. More recently, in the CHANCE trial [Wang Y et al. N Engl J Med. 2013], > 2500 Chinese patients with nondisabling stroke or TIA and with an ABCD2 score of ≥ 4 were treated with clopidogrel (300 mg loading dose, then 75 mg/d for 90 days) plus aspirin (75 mg/d for 21 days). When compared with treatment with aspirin alone, dual antiplatelet therapy reduced the risk of stroke at 90 days by 32% without significantly increasing the rate of bleeding.
In the United States, the ongoing phase 3 POINT trial [NCT00991029] will randomly assign patients within 12 hours of TIA to receive clopidogrel (600 mg loading dose) plus aspirin (50 to 325 mg) followed by maintenance clopidogrel (75 mg/d) or placebo for 90 days. Dr Asimos recommended not changing clinical practice in the United States regarding early antiplatelet therapy until the results of the POINT trial are available late in 2016.
In 2013, the American College of Emergency Physicians (ACEP) published a clinical policy recommending that tissue plasminogen activator (tPA) be offered or considered in patients with acute ischemic stroke in those who meet the National Institute of Neurological Disorders and Stroke inclusion criteria [Edlow JA et al. Ann Emerg Med. 2013]. Widespread controversy prompted the formation of a Clinical Policies tPA subcommittee [Cantrill S. ACEP Now. 2014]. The subcommittee conducted an updated literature search and reviewed open comments received from ACEP members. The subcommittee's recommendation was to update the tPA policy. This recommendation was approved in June 2014 by the ACEP board.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.