

Summary
The management of rheumatoid arthritis (RA) requires effective strategies for optimizing drug selection and application. This article provides a review of the efficacy of novel compounds, the treat-to-target approach, and updated recommendations from the European League Against Rheumatism [Smolen JS et al. Ann Rheum Dis 2013]. Also discussed are considerations when initiating DMARDs during vaccinations.
- Vaccinations
- Rheumatoid Arthritis
- Vaccinations
- Rheumatology
- Rheumatoid Arthritis
The management of rheumatoid arthritis (RA) requires effective strategies for optimizing drug selection and application, stated Daniel Aletaha, MD, MSc, Medical University of Vienna, Vienna, Austria, who provided a review of the efficacy of novel compounds, the treat-to-target (T2T) approach, and updated recommendations from the European League Against Rheumatism (EULAR) [Smolen JS et al. Ann Rheum Dis 2013].
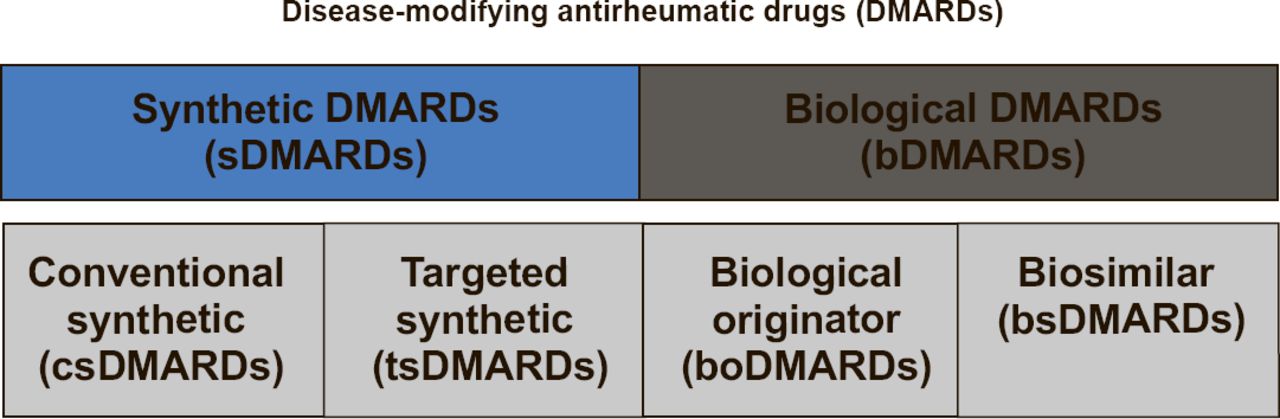
A new, refined classification of disease-modifying antirheumatic drugs (DMARDs) from EULAR underscores the large range of treatment choices (Figure 1). The American College of Rheumatology (ACR) 20/50/70 responses to newer DMARDs in some populations in clinical trials is shown in Table 1; Prof. Aletaha stated that the ACR criteria, highlight the population as the determinant of efficacy, and not the drug.

New EULAR Classification of DMARDs
ACR 20/50/70 Response to Newer DMARDs
T2T is a key strategy for treating RA, comprised of establishing the target, assessment, and adjustment of treatment as needed to reach the target [Smolen JS et al. Ann Rheum Dis 2010]. Notably, the T2T strategy requires elimination of lengthy (>6 months) segments of ineffective treatment, said Prof. Aletaha. This is based on an updated recommendation from EULAR [Smolen JS et al. Ann Rheum Dis 2013] that calls for frequent monitoring in active disease (every 1 to 3 months) and treatment adjustment if there is no improvement by at most 3 months after treatment initiation or if the target has not been reached by 6 months.
Other EULAR recommendations highlighted by Prof. Aletaha were as follows:
-
▪ For DMARD-naïve patients, a conventional synthetic DMARD (csDMARD) therapy (mono or combination), regardless of glucocorticoids (GCs) is recommended
-
▪ When target was not achieved with initial DMARD strategy, in the absence of poor prognostic factors, consider a change to another csDMARD; in the presence of poor prognostic factors, consider addition of a biological DMARD (bDMARD)
-
▪ When the first bDMARD fails, change to another bDMARD; a failed tumor necrosis factor (TNF)-inhibitor can be replaced with another TNF-inhibitor or bDMARD with different mode of action
-
▪ Tofacitinib may be considered after bDMARD failure
-
▪ For patients with insufficient response to methotrexate (MTX) or another csDMARD, with or without GC, combination therapy with MTX and a bDMARD (TNF-inhibitors, abatacept, tocilizumab, or under certain circumstances rituximab) should be initiated
There are no clinical differences between first-line combination therapy with biologicals and a step-up approach to biologicals, based on results from the newly published multinational randomized OPTIMA trial [Smolen JS, Emery P et al. Lancet 2013]. The outcomes for disease activity score and remission were numerically similar for patients whose initial treatment was adalimumab plus MTX or if the initial treatment was MTX with the addition of adalimumab if an insufficient response to MTX monotherapy occurred.
Dose reduction or stopping TNF-inhibitors may be an option for some patients. At Week 78 of the OPTIMA trial, remission rates were only ∼8% higher and the disease activity score ∼7% higher in the patients who continued adalimumab plus MTX compared with those who stopped treatment after achieving a low disease activity at Week 62. The PRESERVE trial showed that patients whose dose of etanercept was reduced from 50 to 25 mg achieved similar rates of remission compared with those taking etanercept 50 mg, both combined with MTX, compared with placebo plus MTX [Smolen JS et al. Lancet 2013]. In patients who are responding well, a valuable approach is dose reduction, said Prof. Aletaha.
CONSIDERATIONS FOR INITIATING DMARDS AND INFECTION PREVENTION
Comorbidities must be evaluated before initiating or changing DMARDs in order to decrease drug-related adverse events. Immunizations are most effective before DMARD therapy is initiated, and patients taking nonbiologic DMARDs (nbDMARDs) or bDMARDs should receive most vaccines, according to Clifton O. Bingham III, MD, Johns Hopkins University, Baltimore, Maryland, USA. The potential risk of live virus vaccines in these immunocompromised patients must be recognized, he stated. Education of patients and providers about the potential for infection with bDMARDs is important to decrease risk.
General screening before staring DMARD therapy should include a medical history, assessment of comorbidities, and determining concomitant medications for potential interactions, allergies, and immunization history. Infection history and risk must be evaluated, including HIV, hepatitis B and C, tuberculosis, and fungal infections. Travel history, both prior and planned, should be taken because of the impact this may have on potential immunization in patients taking DMARDs. Social history, including alcohol to account for effects on liver function testing, and family planning and sexual history are important considerations. Equally important is educating the patient to inform their physician about new medications or medical events or problems.
Cardiovascular screening for specific DMARDs should include hyperlipidemia (in relation to tocilizumab, tofacitinib), chronic heart failure (TNF-inhibitors), arrhythmia (zoledronic acid), and tenuous cardiac status (rituximab). Pulmonary screening is advised for interstitial lung disease and fibrosis (MTX), chronic obstructive pulmonary disease (abatacept), and granulomatous infection and exposure (TNF, other biologics). Gastrointestinal screening includes peptic ulcer disease (steroids), diverticulitis (tocilizumab, tofacitinib), and liver function (MTX, leflunomide, tocilizumab, tofacitinib, TNFs). Regarding renal disease, a creatinine clearance >30 mL/min is needed because of the required dose adjustment for MTX and tofacitinib. Hematologic considerations are neutropenia (MTX, leflunomide, TNF, tocilizumab, tofacitinib, anakinra), lymphopenia (tofacitinib), and thrombocytopenia (MTX, tofacitinib).
Patients with RA have an increased risk of infection, and most DMARDs have a risk for infection. A patient's specific history of infection is important for DMARD selection. Recurrent bacterial infection is a concern with most DMARDs. Fungal and mycobacterial infection and exposure are important regarding TNF and other biologics. HIV is a consideration for all DMARDs, except sulfasalazine and hydroxychloroquine. For hepatitis B and C, the use of MTX, leflunomide, biologics, and tofacitinib is cautioned or contraindicated. Neurologic concerns with TNF include demyelination, multiple sclerosis, and optic neuritis.
A concern of all rheumatologists about using immunomodulatory therapies is the risk of malignancy, and the effect on patients with an underlying or history of malignancy. TNF inhibitors and ustekinumab have warnings about basal or squamous cell skin cancer. Solid tumors are a concern for all bDMARDs, except potentially rituximab. Lymphoproliferative disease is a concern with MTX, TNF, tofacitinib, and possible other bDMARDs except rituximab.
Optimal immunological memory is achieved before the initiation of DMARDs, and this is the best window of opportunity to achieve benefit. Caution is needed with live virus vaccines, because the attenuated viruses used as part of immunizations can become pathogenic and cause illness in immunosuppressed patients, said Dr. Bingham. Live virus can be shed and detectable for up to 3 weeks after vaccination. Live virus vaccines that are a concern for patients on immunomodulatory therapy include varicella and herpes zoster; measles, mumps, and rubella; yellow fever, rotavirus, intranasal influenza, oral polio, vaccinia (smallpox), and some rabies vaccines outside the United States. Live bacteria include Bacillus Calmette– Guérin tuberculosis vaccine and the oral typhoid vaccine. Although the response in RA patients may be blunted, many patients achieve protective titers, and thus immunization is warranted, except for the live virus vaccines while taking most DMARDs.
Patient education is a key step to reduce drug-related infectious morbidity. Patients should be advised to purchase a thermometer and observe a low threshold when calling their physician. Patients need to understand that trimethoprim sulfamethoxisol interacts with MTX, and when to hold the bDMARDs. Dr. Bingham stated that at his clinic the traditional nonbiologic DMARDs (MTX, leflunomide, sulfasalazine, and hydroxychloroquine) are not held for most infections.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.