

Summary
This article gives an overview of warfarin in stroke prevention compared with the new oral anticoagulants (NOACs). While warfarin has been widely used in stroke prevention, it has less desirable attributes such as difficulties in achieving the correct therapeutic dose, interpatient variability, medication compliance, food and drug interactions, and variability amongst generic formulations. Also discussed are the benefits of warfarin versus NOACs in secondary prevention, and a brief summary of patient considerations with NOACs based on clinical trial data.
- Thrombotic Disorders
- Neurology
- Thrombotic Disorders
Gregory J. del Zoppo, MS, MD, University of Washington, Seattle, Washington, USA, gave an overview of warfarin in stroke prevention compared with the new oral anticoagulants (NOACs). While warfarin has been widely used in stroke prevention, it has less desirable attributes such as difficulties in achieving the correct therapeutic dose, interpatient variability, medication compliance, food and drug interactions, and variability amongst generic formulations. NOACs include the direct thrombin inhibitor dabigatran and the factor Xa inhibitors apixaban and rivaroxaban. These drugs have been studied for stroke prevention in patients with nonvalvular atrial fibrillation (AF), as summarized in Table 1.
Overview of Newer Oral Anticoagulant Clinical Trials
All 4 studies included patients with and without prior transient ischemic attack (TIA) or stroke. Prespecified, post hoc analyses have been published for 3 of the 4 studies in an attempt to evaluate secondary prevention [RE-LY: Diener HC et al. Lancet Neurol 2010; ARISTOTLE: Granger CB et al. N Engl J Med 2011; Easton JD et al. Lancet Neurol 2012; ROCKET AF: Hankey GJ et al. Lancet Neurol 2012]. Whether or not the primary events were adjudicated is a limitation of the post hoc analyses. When reviewing the evidence of secondary prevention from the aforementioned studies, all had similar outcomes and safety results that paralleled the primary prevention findings but were not as significant. While this suggests that there might be efficacy in patients who have already had a primary event, Prof. del Zoppo noted that the outcomes do not prove this hypothesis.
Alan Go, MD, Kaiser Permanente, University of California, and Stanford University, San Francisco, California, USA, presented benefits of warfarin versus NOACs in secondary prevention. For patients who have already had a stroke, the goal remains “optimizing benefit-to-harm ratio with whatever strategy we choose at that point,” said Dr. Go.
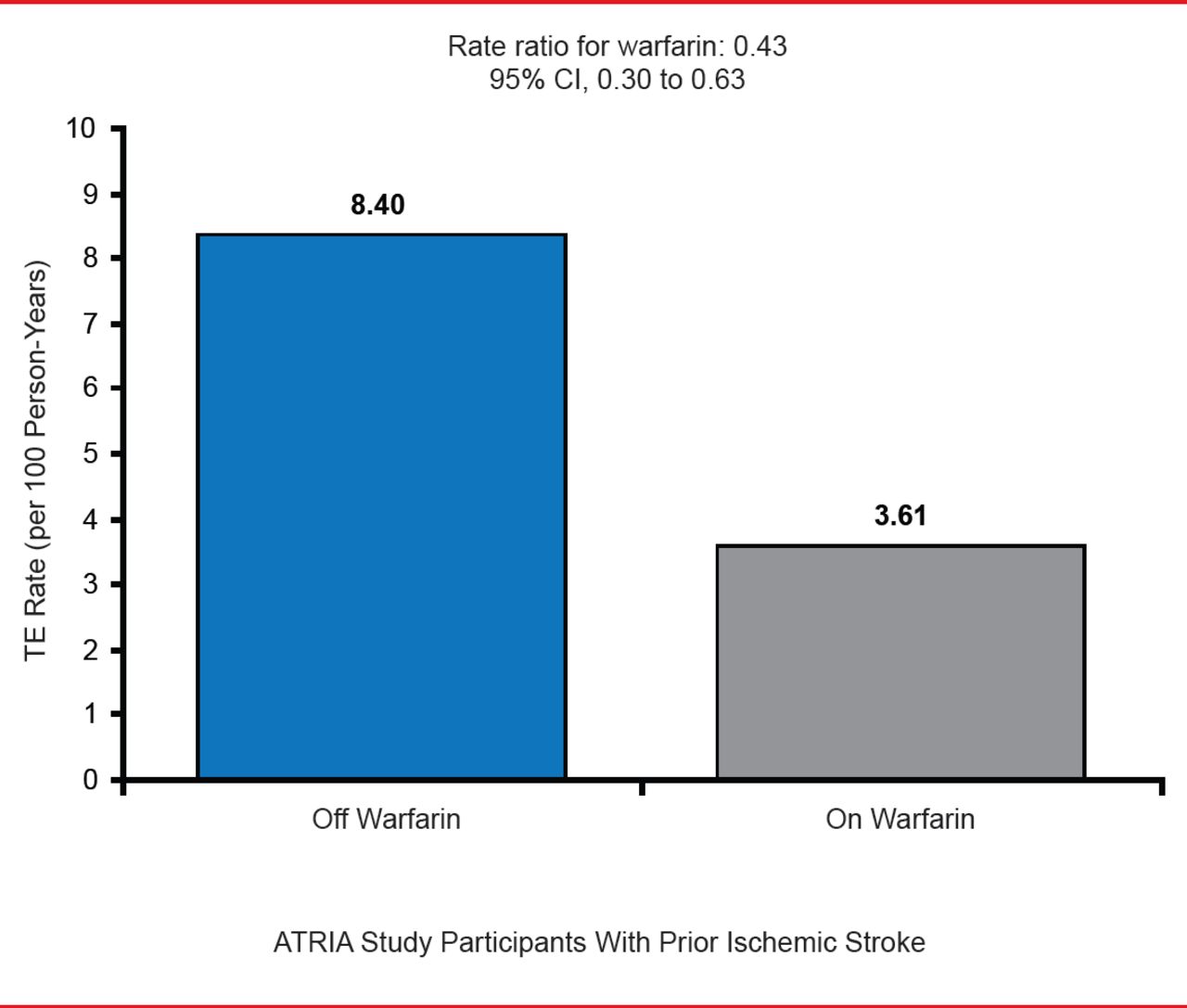
In the Anticoagulation and Risk Factors in Atrial Fibrillation study [ATRIA] (n=13,559), warfarin decreased the risk of a subsequent thromboembolic event in patients with a documented ischemic stroke (Figure 1). However, the risk of death by intracranial hemorrhage is greater in patients taking warfarin (RR, 1.5; 95% CI, 1.1 to 2.0) [Fang MC et al. Stroke 2012].
While the regular monitoring required for use of warfarin may be an inconvenience, Dr. Go believes this is an advantage since patients are seen regularly, problems may be identified earlier, and patient compliance can be assessed. Once-daily dosing may help with patient compliance, compared with the twice-daily dosing of dabigatran and apixaban. Because it has been in use for so long in a real-world setting, a great deal of safety data has been gathered for warfarin.

Effectiveness of Warfarin for Secondary Prevention in Atrial Fibrillation
AF=atrial fibrillation; TE=thromboembolic.
Reproduced with permission from A Go, MD.
Hans-Christoph Diener, MD, PhD, University Hospital, Essen, Germany, gave a brief summary of patient considerations with NOACs based on clinical trial data. The relative efficacy and safety of rivaroxaban or apixaban versus warfarin were consistent in both elderly and younger patients. However, if using dabigatran, a lower dose (110 mg BID, where approved) should be used in patients aged >75 years with a higher risk of bleeding [Eikelboom JW et al. Circulation 2011; Granger CB et al. N Engl J Med 2011; Halperin JL et al. Stroke 2012 (abstr 148)]. In terms of renal function, NOACs appear to be efficacious in a creatinine clearance range of 30 to 50 mL/min but bleeding risk may increase [Connolly SJ et al. N Engl J Med 2009; Eikelboom JW et al. Circulation 2011; Granger CB et al. N Engl J Med 2011]. It is therefore important to carefully monitor older patients at risk of renal impairment or fluid loss, as a reduction in the NOAC dose may be needed.
Patients with a prior gastrointestinal bleed may be anticoagulated with NOACs if the source of bleeding has been identified. The lower dose of dabigatran (110 mg BID) should be used in patients aged >75 years with a history of lower gastrointestinal bleed [Eikelboom JW et al. Circulation 2011]. For patients at high risk of ischemic stroke and moderate risk of cerebral bleeding, “the novel anticoagulants are clearly preferred over warfarin because they have the lower risk,” said Prof. Diener [Ntaios G et al. Stroke 2012]. The question of when to initiate therapy remains unanswered. In all of the NOAC trials, patients could not be randomized in the initial 7 to 14 days after an event. “We have no data whatsoever on this issue. What we definitely need is a prospective registry,” said Prof. Diener. He advises to start NOAC therapy on Day 1 of a transient ischemic attack, 3 days after onset in mild strokes, 6 days later in moderate strokes, and 12 days later in severe strokes.
Triple therapy (aspirin, anticoagulation, and clopidogrel) should be avoided in patients with AF and carotid stenosis as the risk of major bleeding is greatly increased [Eikelboom JW et al. Circulation 2011; Dans AL et al. Circulation 2013]. For this reason, Prof. Diener believes these patients should undergo surgery but not stenting to avoid triple therapy. There is no benefit to combination therapy with warfarin and aspirin in patients with stable coronary heart disease, but the bleeding risk is increased with the combination therapy. While the 3 NOACs are effective in preventing deep vein thrombosis after acute stroke, low-molecular-weight heparin should be stopped 24 hours after starting therapy with a NOAC.
Anticoagulation is contraindicated in patients with advanced small vessel disease, gait apraxia, and frequent falls. Patients with cognitive impairment without severe small vessel disease are candidates for anticoagulation if a caregiver can ensure compliance. Overall, NOACs provide clinicians with additional treatment options. However, all 3 presenters agreed that more long-term safety data is needed to guide physicians in selecting optimal treatment.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.