

Summary
Approximately 20% of all ischemic strokes are caused by cardiac embolism [Freeman WD et al. Neurotherapeutics 2011]. Cardioembolic strokes are disproportionately more disabling than strokes caused by nonembolic mechanisms due to occlusion of larger intracranial arteries and larger ischemic brain volume. This article discusses on advances in cardiac imaging, prolonged rhythm monitoring for detection of silent atrial fibrillation (AF), the potential use of biomarkers to improve identification of cardiogenic embolism, as well as the cost-effectiveness of screening patients for AF and selection of patients for screening for AF for secondary stroke prevention
- Imaging Modalities
- Ischemia
- Cerebrovascular Disease
- Cardiac Imaging Techniques
- Neuroimaging
- Imaging Modalities
- Neurology
- Ischemia
- Cerebrovascular Disease
- Cardiac Imaging Techniques
- Neuroimaging
Approximately 20% of all ischemic strokes are caused by cardiac embolism [Freeman WD et al. Neurotherapeutics 2011]. Cardioembolic strokes are disproportionately more disabling than strokes caused by nonembolic mechanisms due to occlusion of larger intracranial arteries and larger ischemic brain volume. Hee Joon Bae, MD, PhD, Seoul National University Bundang Hospital, Gyeonggi-do, Korea, reported on advances in cardiac imaging and ultrasound.
The European Association of Echocardiography recommends transesophageal echocardiography (TEE) and transthoracic echocardiography when symptoms that could be caused by a cardiac etiology are present, including syncope, cerebrovascular events, and transient ischemic attack (TIA) [Pepi M et al. Eur J Echocardiogr 2010]. However, TEE has several shortcomings: it is semi-invasive, it is difficult to evaluate the aortic arch due to a blind spot, it is not readily available 24 hours a day, and there is a high procedure failure rate in acute stroke patients [Ko SB et al. Cerebrovasc Dis 2010].
Cardiac multidetector computed tomography (MDCT) offers some benefits that TEE does not. It is an electrocardiogram (ECG)-gated scan that provides a better view of the ascending aorta, only takes a short amount of time to scan the patient, is available 24 hours a day, and is less dependent on a patient's condition.
In a study of 75 patients who underwent both cardiac MDCT and TEE following acute ischemic stroke, cardiac MDCT identified a high-risk intracardiac embolic source in 8 patients compared with one identified by TEE. Cardiac MDCT identified 20 patients with extracardiac embolic sources compared with 7 identified by TEE [Ko SB et al. Cerebrovasc Dis 2010].
Prof. Bae concluded that MDCT may provide therapeutic opportunity with respect to the management of cardioembolism and cryptogenic stroke. In addition, cardiac MRI is emerging as another potential option for detection of cardioembolism.
Alejandro Rabinstein, MD, Mayo Clinic, Rochester, Minnesota, USA, presented information on prolonged rhythm monitoring for detection of silent atrial fibrillation (AF) in patients with a previous cryptogenic stroke. AF, which is commonly observed in patients with ischemic stroke and TIAs, increases the risk of ischemic stroke by 5-fold [Seet RCS et al. Circulation 2011]. Paroxysmal AF (PAF) can be difficult to detect due to its asymptomatic, brief, and episodic nature.
To better understand the role of PAF in patients with cryptogenic stroke, the Detection of Occult Paroxysmal Atrial Fibrillation After Stroke Using Prolonged Ambulatory Cardiac Monitoring trial [NCT01325545] enrolled 132 patients within 3 months of an ischemic stroke without documented AF. It was a case-control study with 66 cases of cryptogenic stroke and 66 control cases with documented stroke causes. Patients were monitored for 3 weeks using the CardioNet Mobile Cardiac Outpatient Telemetry system.
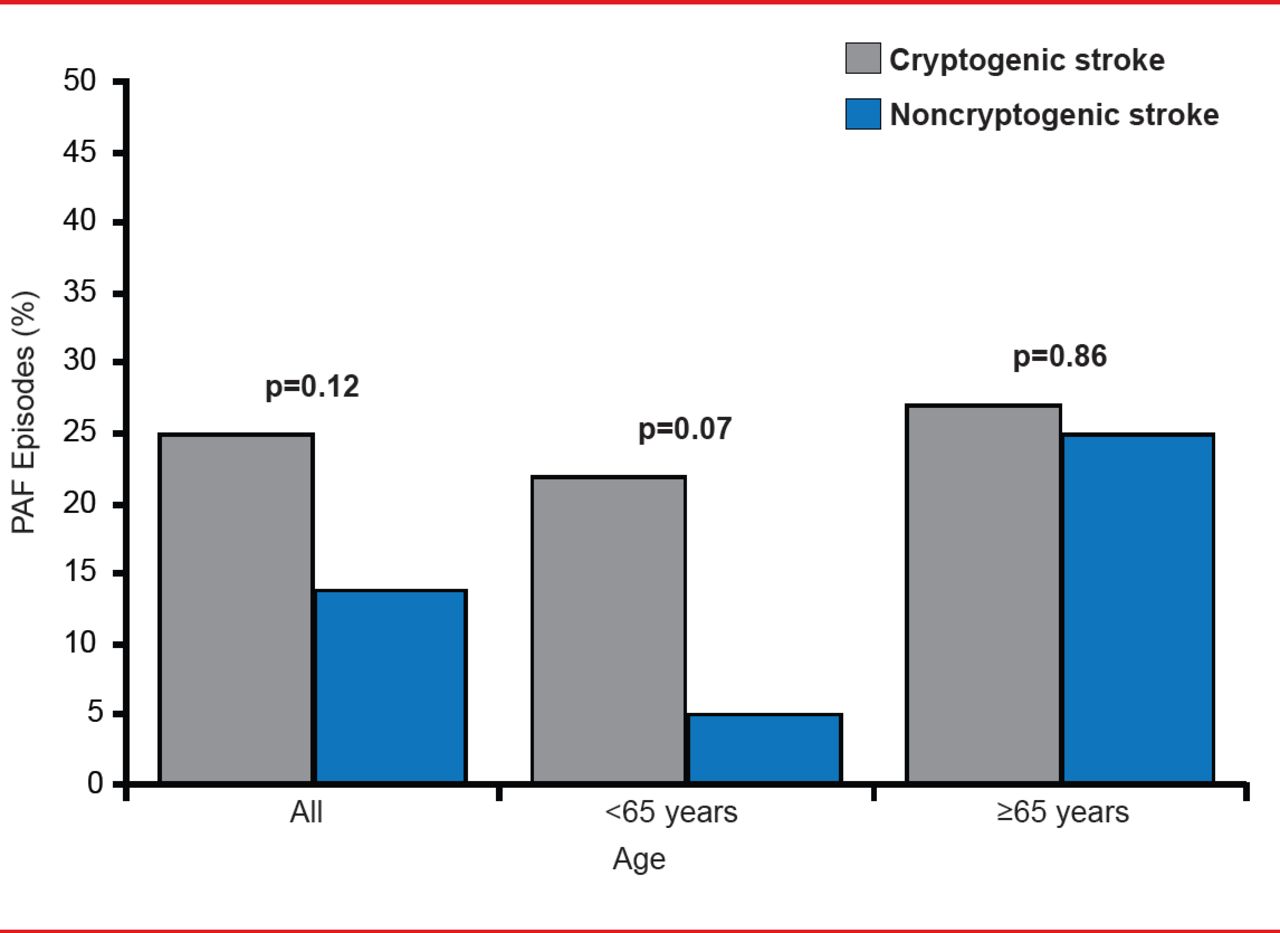
The primary endpoint was detection of PAF independently confirmed by blinded cardiologists. In the final analysis, 16 (25%) of 64 cryptogenic cases had PAF compared with 9 (14%) of 64 control cases, indicating that there was not a significant difference in the occurrence of PAF in cryptogenic stroke cases (p=0.12). Only 3 cryptogenic cases and 2 control cases had PAF episodes lasting >30 seconds. In noncryptogenic stroke cases, PAF was more common in patients aged >65 years (p=0.86) than in patients aged <65 years (p=0.07; Figure 1).
Dr. Rabinstein said that although AF is a major cause of stroke, “it is unclear whether PAF detected by the new prolonged ambulatory methods has the same pathogenic significance” as AF detected by ECG.
Frank Sharp, MD, University of California, Davis, California, USA, reported on the potential use of biomarkers to improve identification of cardiogenic embolism.
RNA from 194 blood samples from 76 acute ischemic stroke patients was analyzed with a microarray to determine genes that distinguish cardioembolic stroke from large-vessel stroke at 3, 5, and 24 hours after stroke onset [Jickling GC et al. Ann Neurol 2010].

PAF Occurrence in Patients With Noncryptogenic Stroke Is Age-Dependent
PAF=paroxysmal atrial fibrillation.
Reproduced with permission from A Rabinstein, MD.
A 40-gene profile differentiated between cardioembolic stroke and large-vessel stroke with >95% specificity and sensitivity. Cardioembolic stroke due to AF could be differentiated from non-AF causes with a separate 37-gene profile with >90% specificity and sensitivity. Genes found to be unique to cardioembolic strokes compared with controls included those involved in renin-angiotensin signaling, thrombopoietin signaling, NF-kB activation, and a cardiac hypertrophy role of nuclear factors of activated T-cells.
In a later study, the cardioembolic stroke gene profiles and gene profiles for arterial and lacunar strokes were used to predict the cause of cryptogenic strokes [Jickling GC et al. Stroke 2012]. RNA from the peripheral blood of 131 patients with cryptogenic stroke was compared with 149 patients with strokes of known cause. Together with infarct location, gene expression predicted 58% of the cryptogenic strokes to be cardioembolic, 18% arterial, 12% lacunar, and 12% unclear etiology.
Dr. Sharp said that these studies were proof-of-principle studies limited by small numbers of subjects, and a large population study is needed to re-derive gene profiles for cardioembolic, large-vessel, and lacunar strokes.
S. Claiborne Johnston, MD, PhD, University of California, San Francisco, California, USA, presented on the cost-effectiveness of screening patients for AF and selection of patients for screening for AF for secondary stroke prevention.
To determine whether it was feasible to monitor all patients with prior TIA or stroke for AF, a cost-effectiveness analysis was run using a systematic review to create inputs and typical cost-utility methods to develop a model [Kamel H et al. Stroke 2010]. The primary outcome was cost per quality-adjusted life year (QALY). Primary results are shown in Table 1. The cost-utility ratio was $13,000 per QALY. Generally, any amount <$50,000 per QALY is considered reasonable for a health intervention, so the results indicate it is cost effective to monitor most patients with a previous TIA or stroke for AF.
Cost-Effectiveness Analysis of Monitoring Patients for Atrial Fibrillation
Dr. Johnson concluded that if certain patients are going to be selected for monitoring, a composite prediction score needs to be developed and validated that takes risk factors for AF into account. These risk factors include age, cryptogenicity, cortical infarct, normotension, brain natriuretic peptide, premature atrial contractions, and heart disease.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.