

Summary
Among other topics, this article discusses showing that catheter ablation guided by complex fractionated atrial electrograms (CFAE) is a viable alternative treatment for atrial fibrillation (AF) in the elderly, and reviewed some of these ablation strategies with a focus on 3D automated CFAE-guided right atrium ablation. The article also presents results from a prospective randomized study that assessed the comparative efficacy of a stepwise ablation approach and a simplified approach consisting of two circumferential pulmonary vein antrum isolations and three linear atrial ablations in patients with persistent AF.
- Interventional Techniques & Devices
- Arrhythmias
- Interventional Techniques & Devices
- Arrhythmias
- Exclusive Article - For home page
- Cardiology
Koonlawee Nademanee, MD, Pacific Rim Electrophysiology Research Institute at White Memorial Medical Center, Los Angeles, California, USA, presented data showing that catheter ablation guided by complex fractionated atrial electrograms (CFAE) is a viable alternative treatment for atrial fibrillation (AF) in the elderly although multiple procedures maybe required.
The study comprised 324 patients (>60% men; mean age 79 years) with symptomatic AF. A total of 261 patients received ablation and 63 no ablation. Long-standing AF was more common (present in 49.4% and 44% of patients in the ablation and no-ablation groups, respectively) than either paroxysmal AF (PAF; 27.2% vs 29%) or persistent AF (PeAF; 23.4% vs 27%). Patients in the ablation group had a mean ejection fraction of 51% and AF duration of 48 months compared with 49% and 43 months in the no-ablation group. Significantly more patients in the ablation group had valvular disease (15%) versus those in the no-ablation group (3%; p<0.01). The aims of the study were to examine the safety and efficacy of AF substrate ablation guided by CFAE and the risks associated with discontinuation of warfarin after ablation. Clinical endpoints were sinus rhythm (SR), death, stroke, systemic emboli, and major bleeding. Radiofrequency ablation continued until AF converted to SR or until all CFAE areas were ablated. Warfarin was continued for 3 months after the ablation and was discontinued only after SR was established and maintained.
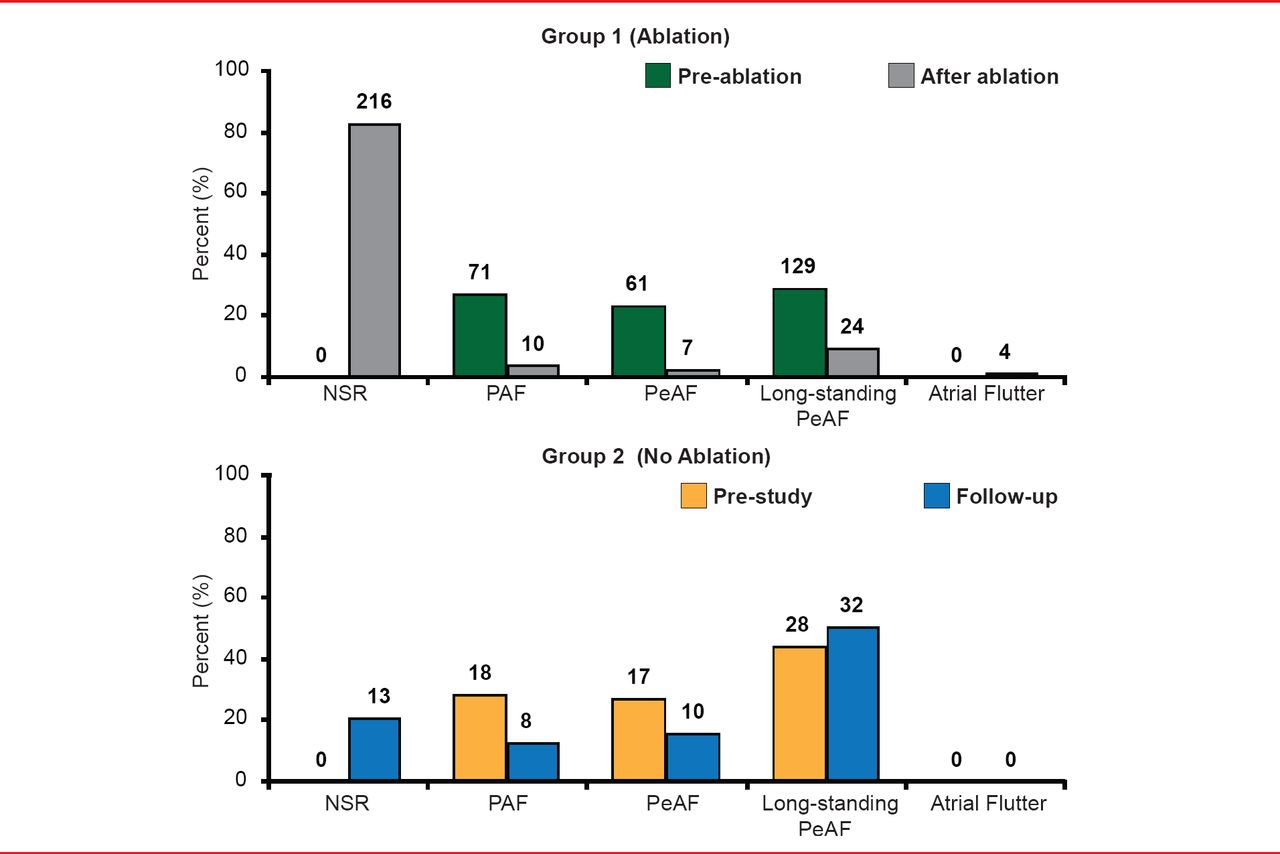
Normal SR was achieved by 80% of patients receiving ablation compared with 20% of those in the no-ablation group (Figure 1).

Effect of Ablation on Atrial Fibrillation
AF=atrial fibrillation; NSR=normal sinus rhythm; PAF=paroxysmal atrial fibrillation; PeAF=persistent atrial fibrillation. Reproduced with permission from K Nademanee, MD.
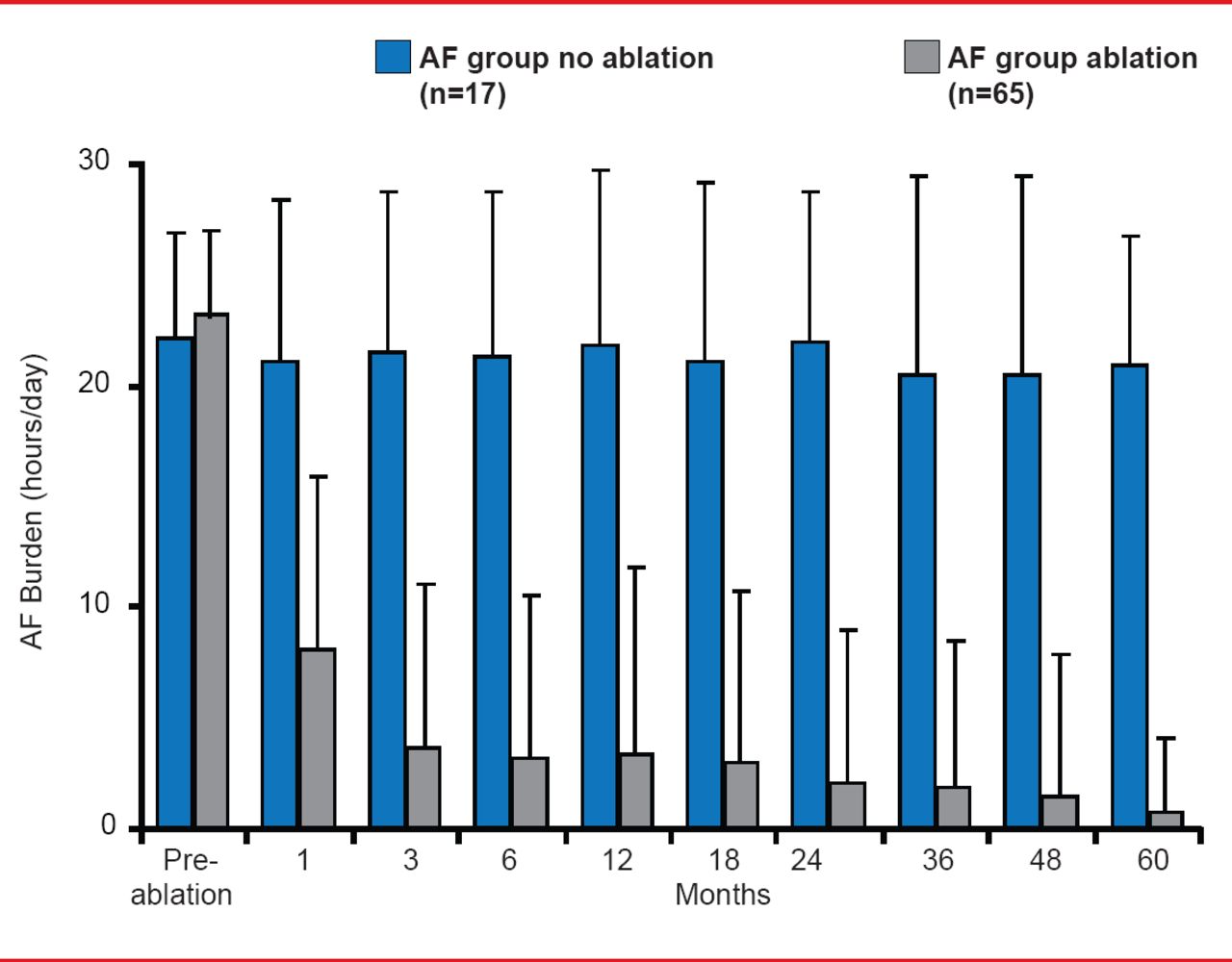
Although the AF burden (defined as the percentage of time a patient is in AF or atrial tachycardia[AT]), was the same for both groups before ablation, but decreased to <10% at 1 month and to ≤1% by 60 months in the ablation group (Figure 2).

Long-Term Effects of Ablation on AT/AF Burden
AF=atrial fibrillation.
Reproduced with permission from K Nademanee, MD.
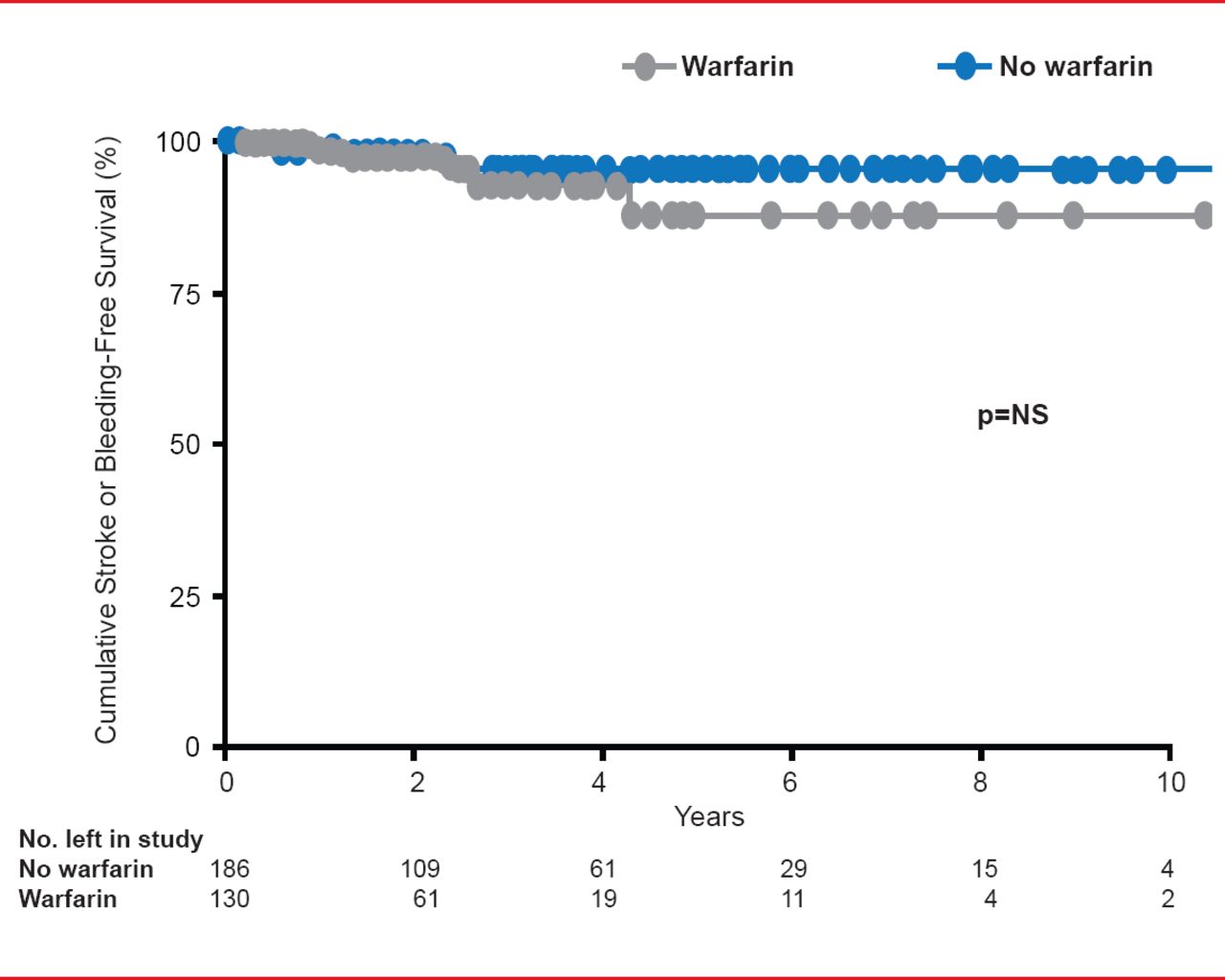
By 60 months post ablation, AF was totally suppressed in >60% of patients. After 3 years, 15.7% (n=34) of patients in the ablation group died compared with 35.5% (n=16) in the no-ablation group (annual morality rate of 4% vs 9.8%; p<0.0001). There was no difference in stroke or bleeding-free survival rates after ablated patients stopped taking warfarin at any time point (Figure 3).

Effects of Warfarin Discontinuation on Stroke or Bleeding Rate
Reproduced with permission from K Nademanee, MD.
AF ablation had a low complication rate. Procedural complications included two strokes (0.8%), four hemopericardium (0.6%), 10 major bleeds at the groin sites (4.0%), and two pulmonary edemas (1%). Further study is warranted to determine the role of ablation in the management of AF in the elderly population.
Patients with PAF receive very effective treatment with left atrium (LA)-based catheter ablation. However, PeAF is more complex and no single strategy has been shown to be uniformly effective. A number of different ablation strategies for PeAF have been used, including pulmonary vein isolation (PVI), targeting of CFAEs, multilinear lesions, and various combinations and modifications of these lesion sets [Kim YH. Circ J 2012]. Other strategies include CFAE-guided ablation, right atrium (RA) septum ablation, Bachman's bundle ablation, mitral valvular annulus (MVA) ablation, and crista terminalis ablation.
Young-Hoon Kim, MD, PhD, Korea University Medical Center, Seoul, South Korea, reviewed some of these ablation strategies with a focus on 3D automated CFAE-guided RA ablation. Results from his studies show that CFAE-guided RA ablation is effective in 50% of the patients in whom AF persisted after PVI and LA CFAE-guided ablation. In addition, after 13.6±8.7 months of follow-up, significantly (p<0.05) more patients were AF or AT-free (68.8%) in the mapped CFAE group than in the anatomical group (50.6%).
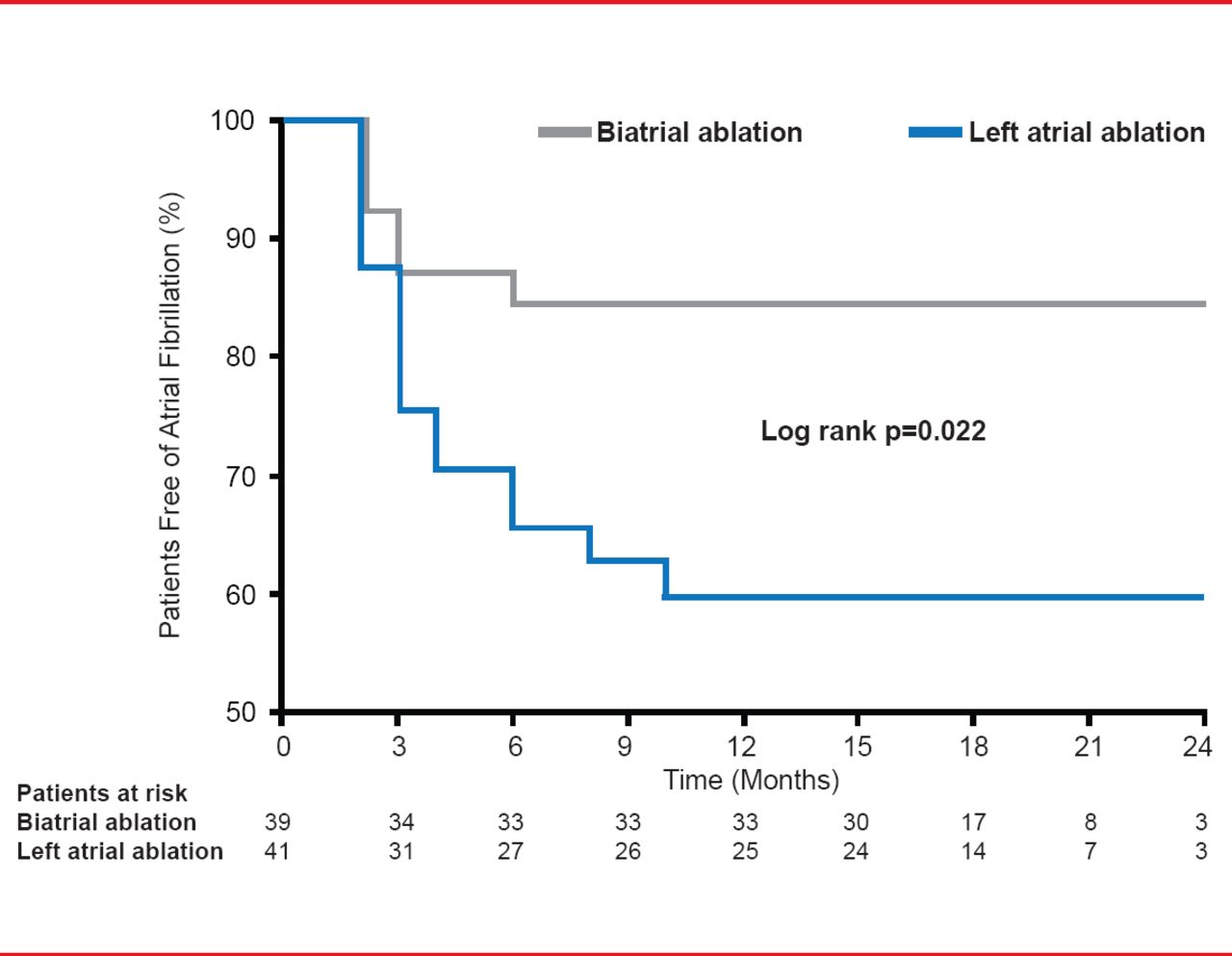
In patients with PeAF, circumferential PVI ablation, combined with linear lesions in the RA, proved more effective than PVI only or PVI plus LA linear lesions, even when both were used with CFAE mapping. AF recurred in 39% of patients in the LA-ablation group and in 15% of patients in the biatrial-ablation group (p=0.022; Figure 4) [Calò L et al. J Am Coll Cardiol 2006].

Biatrial Ablation Has a Significantly Higher Success Rate Than LA Ablation Alone in PAF and PeAF
Reproduced with permission from K Nademanee, MD.
The RA drives AF in ∼20% of PeAF [Hocini M et al. J Am Coll Cardiol 2010]. The addition of an RA lesion to an extended LA lesion set does not improve efficacy, but it does increase the rate of pacemaker placement for sinus dysfunction. Adding an LA appendage lesion may confer additional efficacy when added to a lesion set that includes PVI plus MVA (Figure 5) [Soni LK et al. J Thorac Cardiovasc Surg 2013].

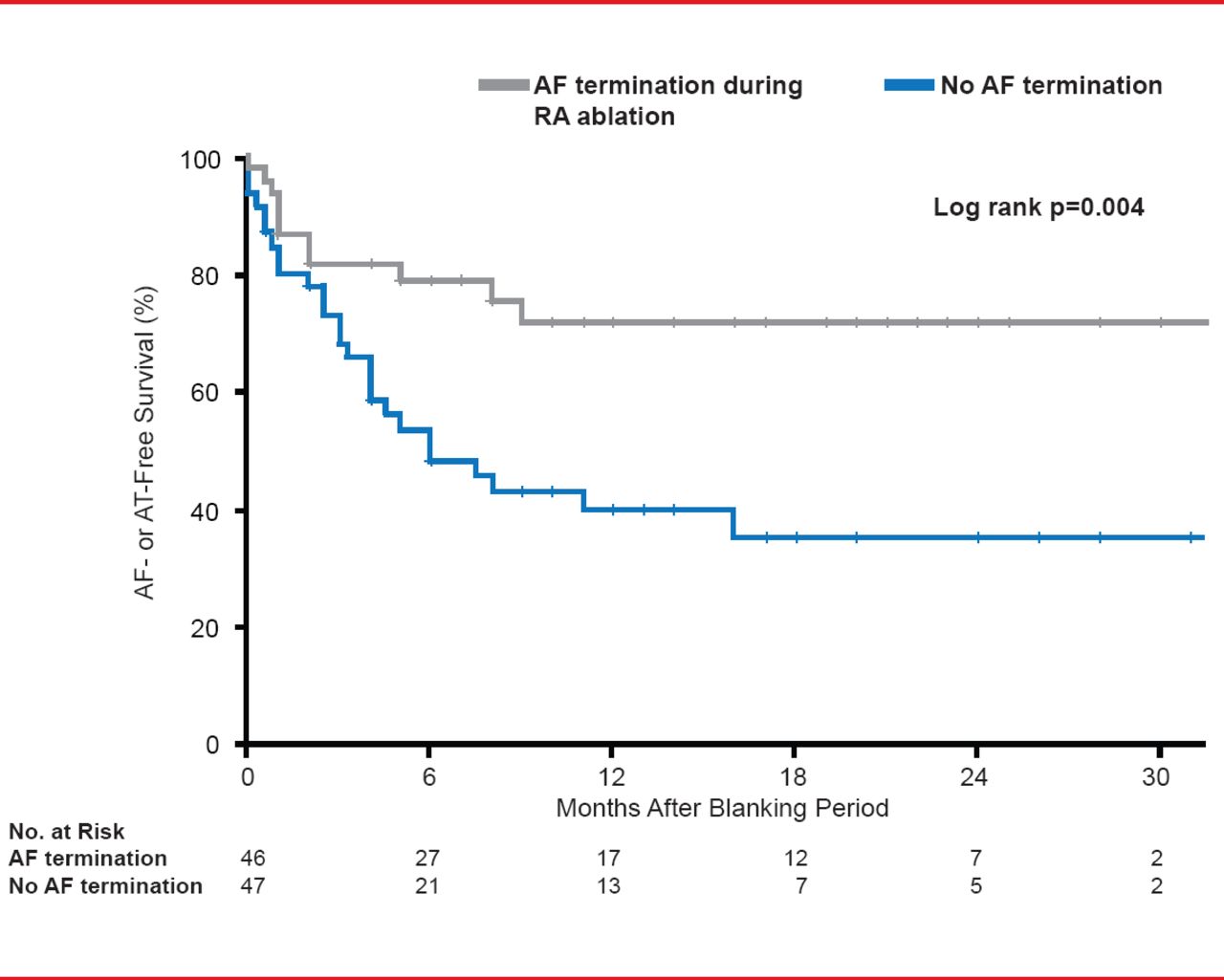
AF- or AT-Free Survival Following RA Ablation
AF=atrial fibrillation; AT=atrial tachycardia; RA=right atrium.
Reproduced with permission from YH Kim, MD, PhD.
RA ablation works best in patients who are refractory to extensive LA ablation. Prof. Kim presented data from an unpublished study in which RA CFAE ablation for sustained AF was performed after PVI/LA CFAE ablation in 97 patients [Chen YL et al. J Cardiovasc Electrophysiol 2013. In press]. AF was terminated in 49% (n=48) of patients and sustained in 51% (n=49) of patients. For those patients with AF termination, 80% experienced AF- or AT-free survival compared with 40% with no AF termination 30 months after the blanking period (Figure 5).
Complications (13/97 patients, 13.4%) of extensive RA ablation using 3D automated CFAE include cardiac tamponade, sinus node dysfunction, transient phrenic nerve paralysis, and atrioventricular block [Chen YL et al. J Cardiovasc Electrophysiol 2013. In press]. Phrenic nerve injury (PNI) is a rare complication (0.48%) of AF ablation. Ablation of the right superior PV, superior vena cava, and LA appendage were associated with PNI [Sacher F et al. J Am Coll Cardiol 2006].
Non-pulmonary vein (NPV) ectopy initiating AF/AT is noted in ∼20% of patients with AF, more often those with non-PAF (NPAF) [Chang HY et al. J Cardiovasc Electrophysiol 2013]. Advanced atrial remodeling is an important mechanism. The most common locations for these triggers are the superior vena cava (6.7%), LA posterior wall (2.7%), and ligament of Marshall (2.7%). Other locations include crista terminalis (2.3%), interatrial septum (1.5%), and the coronary sinus ostium (0.8%), but there also some triggers outside of PVs. Li-Wei Lo, MD, Taipei Veterans General Hospital/National Yang-Ming University, Taipei, Taiwan, reported that AF originating from the NPV had a higher recurrence rate after catheter ablation.
It has been noted that the origin sites of the NPV ectopies are at the same location as those of the atrial continuous CFAEs [Lo LW et al. J Cardiovasc Electrophysiol 2009], thus limited ablation targeting all atrial continuous CFAEs could eliminate AF. The current study included 660 consecutive patients (aged 54±11 years; 68% men) who had undergone catheter ablation for AF. Group 1 (n=132) had AF initiating from the NPV and Group 2 (n=528) from the PV triggers only [Chang HY et al. J Cardiovasc Electrophysiol 2013]. Patients in Group 1 were younger (p<0.001), more likely to be female (p=0.049), and had a higher incidence of NPAF (p<0.001). In addition, right atrial enlargement was larger and the biatrial substrates were worse.
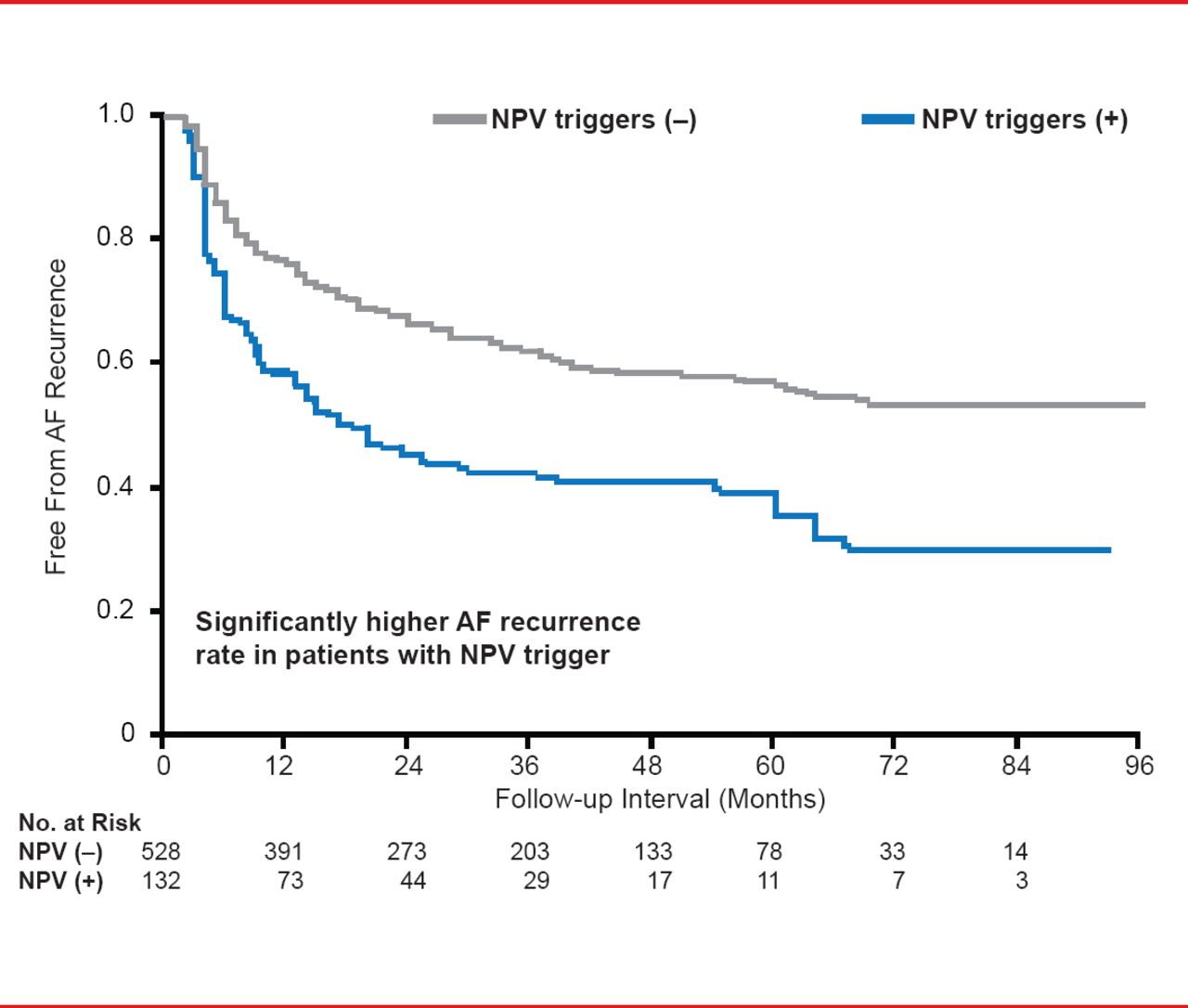
There was a significantly (p<0.001) higher rate of AF recurrence in Group 1 patients with NPV triggers compared with patients with AF originating from the PV alone (57.6% vs 38.8%; Figure 6).

Long-Term Outcome After Ablation
AF=atrial fibrillation; NPV=nonpulmonary vein.
Reproduced with permission from YH Kim, MD, PhD.
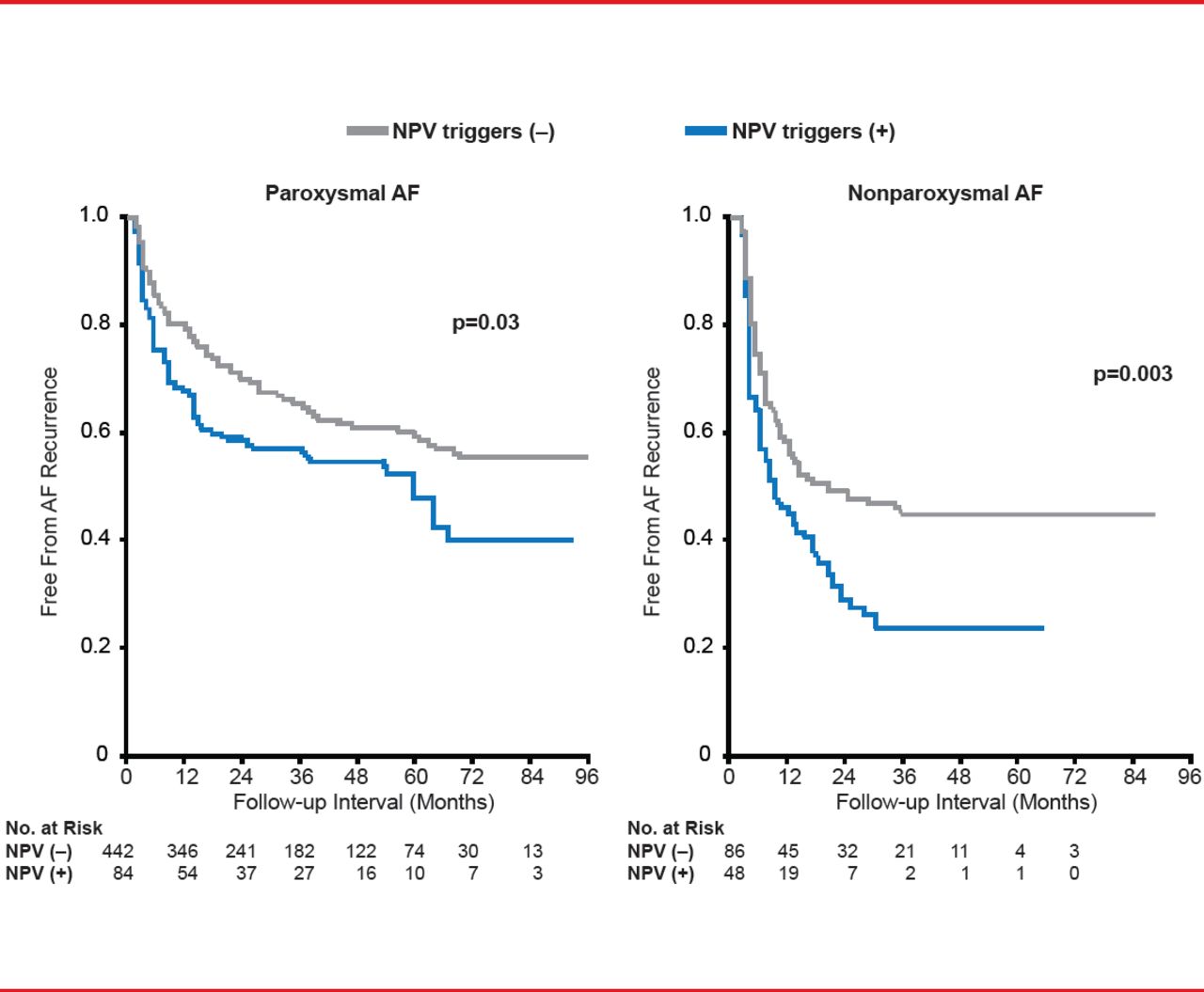
Independent predictors of AF recurrence were NPV triggers (p<0.001; HR, 2.0; 95% CI, 1.4 to 2.85); NPAF (p=0.021; HR, 1.55; 95% CI, 1.07 to 2.24); larger LA diameter (p=0.002; HR, 1.04; 95% CI, 1.02 to 1.07); and worse LA substrate (p=0.028; HR, 1.3; 95% CI, 1.03 to 1.64) [Chang HY et al. J Cardiovasc Electrophysiol 2013]. At 96 months, patients with AF originating from the NPV presented with worse outcomes (AF recurrence rate: 46.4% vs 36.2%; p=0.03 [Figure 7A] and 77.1% vs 52.3%; p=0.003 [Figure 7B]).

Long-Term Outcome in PAF and NPAF Patients
AF=atrial fibrillation; NPAF=nonparoxysmal atrial fibrillation; NPV=non-pulmonary vein; PAF=paroxysmal atrial fibrillation.
Reproduced with permission from LW Lo, MD.
The recurrence rate between patients with RA and LA NPV triggers was similar [Chang HY et al. J Cardiovasc Electrophysiol 2013]. Prof. Lo stated that the AF recurrence rates in NPV patients is ∼20% and might be higher in long-lasting PeAF, which could lead to greater degree of atrial remodeling. There is an increase incidence of NPV triggers as the number of ablation procedures increases, but PV initiating AF remains the major course of AF recurrences. The best procedural strategy is yet to be determined.
Jiang-Zeng Dong, MD, Ahnzen Hospital, Capital Medical University, Beijing, China, presented results from a prospective randomized study that assessed the comparative efficacy of a stepwise ablation approach and a simplified approach consisting of two circumferential PV antrum isolations and three linear atrial ablations (2C3L) in patients with PeAF. The study included patients aged >18 to <80 years (mean age ∼56 years and ∼50% men) with symptomatic PeAF (two electrocardiogram-documented episodes of AF at least 7 days apart, within the last 3 months) that was refractory to antiarrhythmic drugs (AADs). The primary study endpoint was freedom from AT and/or organized ATs (OATs) off AADs at least 1 year after a single-ablation procedure. Any AF or AT episode that lasted for >30 seconds beyond the blanking period (the first 3 months post ablation) was defined as a recurrence.
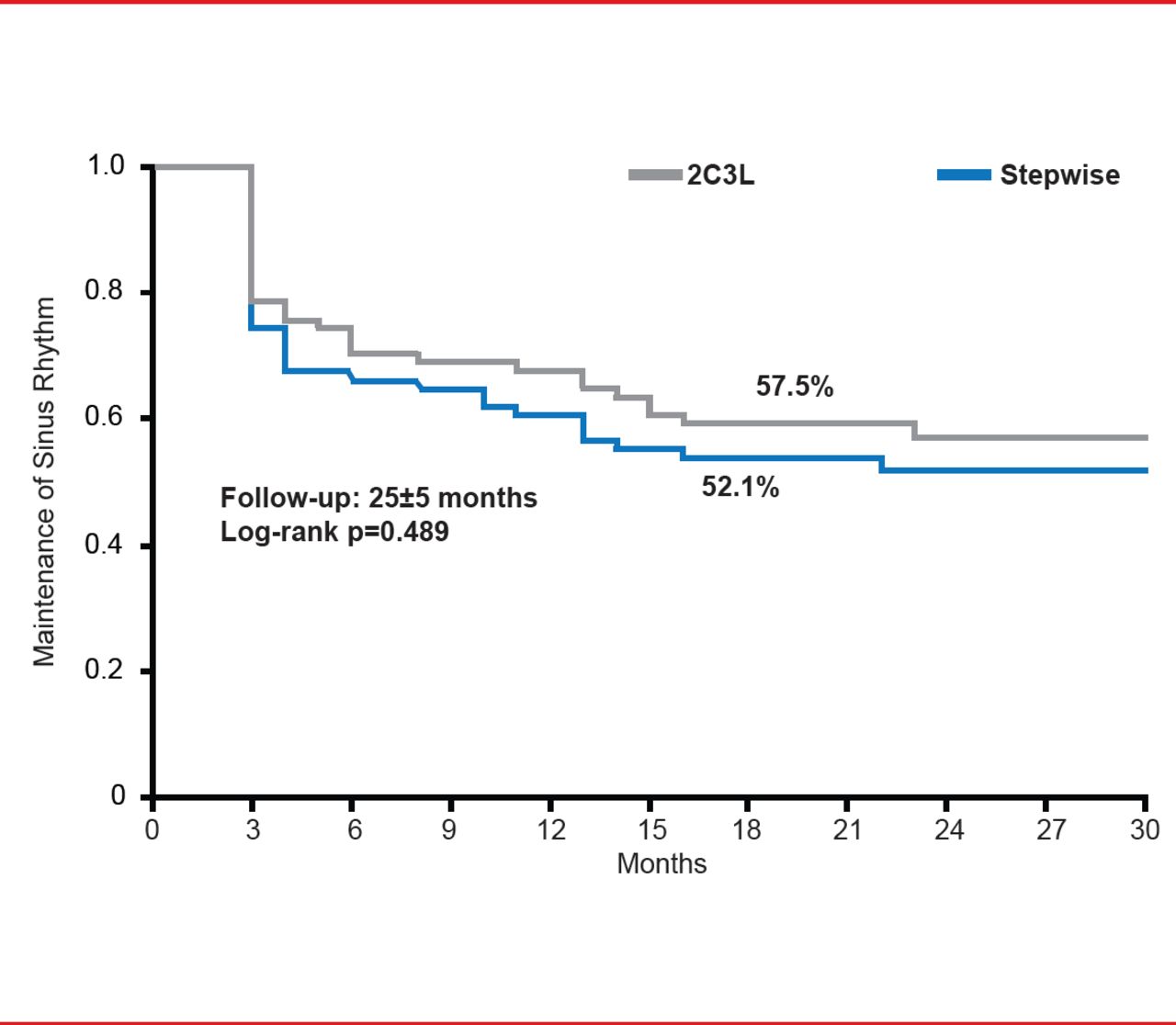
Subjects were randomly assigned to receive either 2C3L (n=73) or stepwise ablation (n=73). At about 2 years, 57.5% patients in the 2C3L group and 52.1% in the stepwise group were in SR without AADs. Twenty-four patients in the 2C3L group received a repeat procedure versus 27 in the stepwise group. There was no difference in SR maintenance after the initial procedure (Figure 8).

Maintenance of SR After Initial Procedure
Reproduced with permission from LW Lo, MD.
Procedure time, fluoroscopy time, and ablation time for the first procedure were significantly shorter for patients receiving 2C3L ablation (all p<0.001). The AF termination rate and number of OATs ablated were significantly lower (both p<0.001) and there were more cardioversions with the 2C3L (1.2) versus the stepwise (0.6; p<0.001). PV antrum isolation was achieved in all patients. Adverse events included one stroke and three femoral hematomas in the 2C3L group and one pericardial tamponade, three incidents of LA appendage activation delay, and four femoral hematomas in the stepwise group.
Compared with the stepwise approach, the 2C3L strategy had similar efficacy and safety but with shorter procedural, fluoroscopy, and radiofrequency energy delivery times.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.