

Summary
There is substantial new evidence that pulmonary rehabilitation (PR) is beneficial for patients with chronic obstructive pulmonary disease and other chronic lung diseases. This article discusses the physiologic approach to PR.
- Chronic Obstructive Pulmonary Disease
- Pulmonary & Respiratory Medicine
- Chronic Obstructive Pulmonary Disease
There is substantial new evidence that pulmonary rehabilitation (PR) is beneficial for patients with chronic obstructive pulmonary disease (COPD) and other chronic lung diseases. Richard Casaburi, PhD, MD, Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Torrance, California, USA, discussed the physiologic approach to PR.
PR is a nonpharmacologic therapy that has emerged as a standard of care for patients with COPD. Evidence shows that it improves exercise tolerance, symptoms of dyspnea, and health-related quality of life better than any other current COPD therapy. It also decreases exacerbations and hospitalizations, reduces depression and anxiety, and improves cognitive function and self-efficacy. The benefits of PR accrue regardless of COPD severity, sex, age, body weight, socioeconomic status, or the presence of comorbidities.
Although its proven effectiveness is broadly accepted, reimbursement strategies prevent many patients from receiving treatment. It is now understood that hospitals need to charge the real cost of the service, including doctors, staff, equipment, and facility use. A recent review reported that PR programs service ≤ 1.2% of the population of patients with COPD, irrespective of the country [Desveaux L et al. COPD. 2014], something that needs to be corrected, Dr Casaburi noted.
A PR therapy program is a comprehensive, multidisciplinary, patient-centered intervention that includes patient assessment, education, chest physical therapy, controlled breathing exercises, exercise training, nutritional therapy, and ongoing psychosocial support. Despite early doubts regarding the effectiveness of exercise training—mostly owing to exercise physiology studies showing little change in aerobic muscle enzymes after exercise—it is now a generally accepted treatment strategy. Endurance exercise training increases mitochondrial numbers, aerobic enzymes, and capillary density and improves muscle efficiency. Effective programs include intense training sessions 3 to 5 times a week, each lasting 30 to 60 minutes, for 6 to 12 weeks. The program can be enhanced with good bronchodilator medication, supplemental oxygen, heliox breathing, interval training, and pressure support ventilation.
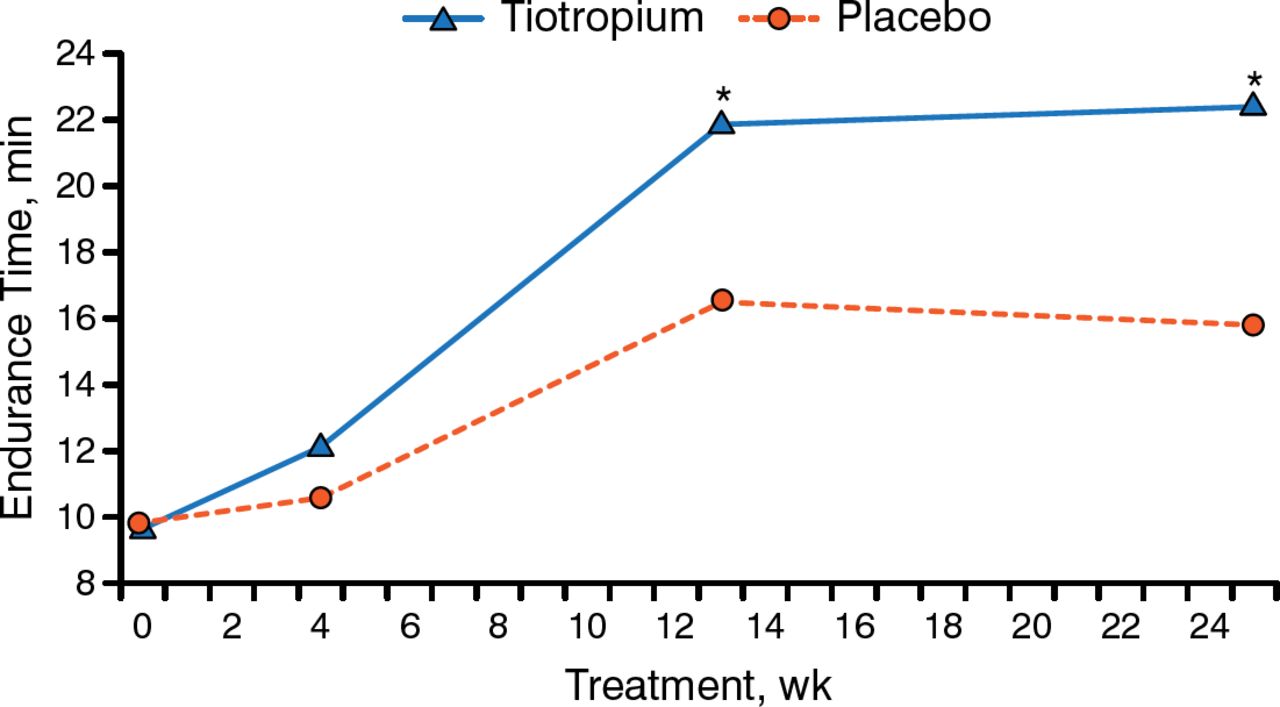
As an example, combining PR with an inhaled anticholinergic bronchodilator (tiotropium) improves airflow and reduces lung hyperinflation in patients with COPD. In a randomized double-blind placebo-controlled trial (n = 93), daily tiotropium supplementation improved endurance time on the treadmill (Figure 1), dyspnea, and respiratory scores and reduced albuterol use; improvements were sustained for 3 months following completion of PR [Casaburi R et al. Chest. 2005].

Tiotropium in Combination With Pulmonary Rehabilitation Improves Exercise Endurance
* P < .05.
Adapted from Casaburi R et al. Improvement in exercise tolerance with the combination of tiotropium and pulmonary rehabilitation in patients with COPD. Chest. 2005;127:809–817. Reproduced with permission from the American College of Chest Physicians.
In a double-blind trial, supplemental oxygen (3 L/min) given to nonhypoxemic patients with COPD undergoing high-intensity training improved exercise capacity when compared with that from compressed air [Emtner M et al. Am J Respir Crit Care Med. 2003]. Patients receiving oxygen had a 40% greater gain in endurance, as determined by constant work rate exercise testing.
In a randomized blinded trial of 82 patients with stable COPD, combining helium with oxygen supplementation (72% He, 28% O2) during exercise increased patients' walking distance by 76.3% and reduced their Borg scores more so than breathing air or other gas combinations [Laude EA et al. Am J Respir Crit Care Med. 2006].
Alternating periods of high-intensity training with lower-intensity training has been shown to improve training outcomes in healthy people, but to date, no COPD studies have found this approach to be superior to constant work rate training, probably because there is no standardized method of raising and lowering work rate. There is, however, some evidence that large-amplitude rapid sinusoidal fluctuation in work rate might be suitable for programs of rehabilitative exercise training in COPD [Porszasz J et al. Exp Physiol. 2013].
An ambulatory ventilation system has been developed that provides inspiratory pressure support triggered by the patient's inspiration. This wearable 1-lb noninvasive open ventilation system, when combined with compressed oxygen, prolongs exercise endurance, reduces respiratory muscle activation (by electromyogram), improves oxygenation, and decreases dyspnea in patients with COPD with exercise-induced hypoxemia [Porszasz J et al. Am J Respir Crit Care Med. 2013].
The second area of study in COPD is dysfunction of the muscles of ambulation, including muscle structure and function, etiology of muscle dysfunction, and interventions to improve muscle function. Skeletal muscle dysfunction in patients with COPD is the result of several conditions, including low muscle mass, poor capillarity, muscle inflammation, and vasoregulatory abnormalities, which lead to early-onset lactic acidosis that worsens dynamic hyperinflation and early muscle fatigue that limits exercise tolerance.
Patients with COPD are susceptible to dynamic hyperinflation. Exercise training may be effective because it decreases dynamic hyperinflation by delaying the attainment of a critically high inspiratory lung volume [Porszasz J et al. Chest. 2005]. This can significantly improve exercise tolerance.
The distinction between strength and endurance training is important. Endurance training promotes aerobic metabolism and is associated with greater quality-of-life improvements; strength training promotes fiber hypertrophy. Both facilitate specific activities of daily living. There are pharmacologic agents that induce changes similar to strength but not endurance training. Muscle weakness in men with COPD may be due the prevalence of low testosterone levels. Testosterone supplementation (100 mg of testosterone enanthate injected weekly) with resistance exercise not only normalized serum testosterone concentration but also significantly (P < .001) improved lean body mass and leg strength more than placebo plus no exercise, testosterone plus no exercise, and placebo plus exercise [Casaburi R et al. Am J Respir Crit Care Med. 2004].
Activity monitors are useful for objective measurement of daily activity in patients with severe COPD, who are known to have low physical activity levels early in disease progression [Troosters T et al. Respir Med. 2010]. Activity level appears to be the best predictor of mortality in COPD patients (P < .001) [Waschki B et al. Chest. 2011].
Going forward, optimization of current treatment, funding for large trials on how to maximize long-term benefits, resolution of the reimbursement issues, training of rehabilitation specialists, and improved access are needed.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.